This week’s questions are all about coping strategies. Traveling, panic attacks, aging, job hunting, emotions, obsessions – it’s a great mix and I think we’re going to come up with a great big pool of potential strategies that we can all draw on when needed.
You know the drill–if you’re on the spectrum, either formally diagnosed or self-identified, you’re welcome to join in. Answer as many or as few as you like. Do it here or anonymously at Survey Monkey.
1. I am wondering if travelling is hard for all Aspies as they age or if it is just me? I like my home at night and my own environment. I prefer to be as close to it as possible…and I get sick or upset if I stay away…my tolerance is two days from home max and two weeks to recover…Does anyone else feel this way? Does it get worse with age or in certain decades? more details here
2. Is liking or disliking foreign travel related to ability to pass for NT at home?
3. Do you experience problems with long flights? If yes, which aspects are most problematic? (which travel stages: e.g. planning, navigating airports, flying, unfamiliar surroundings at the destination etc – and which problematic factors: e.g. sensory overload, executive function issues, anxiety / panic attacks etc) How do you cope with long flights? (what are your coping strategies)
4. How do you cope with panic attacks in unavoidable situations that you can’t leave, such as during flights?
5. Do you find yourself getting more autistic as you get older? Did your coping strategies improve with age due to experience or psychological assistance (I shy away from the word ‘treatment’) or did they deteriorate over time because of a decrease in overall energy?
6. How do you cope with strong emotions, especially strong negative emotions, especially if you’re also alexithymic? How do you support someone going through a very difficult time emotionally (nothing practical to be done)? How do recognise what the feelings are, and how do you respond in a way that comforts the person?
8. A question that is specifically for people who menstruate: do you notice changes during your menstrual cycle. With changes I mean changes in sensory perception, abilities to cope and/or compensate, EF, etc.
9. If you’ve been heavily obsessing about an interest for a while do you find you have to have a short break from it because it has got too intense?
10. Has anyone taken concerta/ritalin/other stimulant drug prescribed to help ADHD type symptoms and reacted very badly to them physically? What effect did it have on you in the short and long term?
At the end of July I embarked on a 30-day experiment, the aptly-named “What Do I Want” experiment. My intention was to report back at the end of August with a neat little of summary of what I’d learned.
Well.
Initially, I thought “what do I want?” meant learning to identify my needs and desires. That sounded intimidating. I had little idea where to begin so I began obsessing over decisionmaking. It was concrete and easy to construct rules around. It was also just scratching the surface of what I needed to be doing.
Wading deeper into the experiment, it became more difficult to separate what I want from other big questions of identity. What I am. How I act. How I think. Who I want to be.
I gradually began to realize that being autistic and alexithymic is only part of what makes “what do I want?” so hard to answer. There is a secondary element at work, an old defense mechanism. Wanting something, getting my hopes up, expressing a preference, letting desire creep in–that makes me vulnerable. To deprivation, to loss, to mockery, to pain. Not wanting feels safe. Ultimately, though, all it gets me is preemptive deprivation. There’s a lot of emptiness in not wanting. Continue reading What I Want→
When I first realized that I was starting to experience the symptoms of menopause, I went in search of more information. The first thing I learned is that I’m not experiencing symptoms of menopause but of perimenopause, the period (heh) before menopause when a woman’s body starts producing less estrogen.
Menopause is the hormonal finish line; perimenopause is the roller coaster ride that gets you there.
There’s plenty of information out there for women experiencing all stages of “the change” but, of course, nearly nothing specifically for autistic women. I don’t know if autistic women experience menopause differently. It sounds like a difficult time for most women, with a lot of variation in symptom type and severity, so it’s hard to say if what I’m experiencing is different from the norm.
What caught my attention, though, is the overlap between some common traits of ASD and symptoms of perimenopause. Many autistic women–myself included–already struggle with sleep problems, temperature regulation, forgetfulness, mood swings (irritability, depression, anxiety), and fatigue.
My biggest question is will this make menopause less difficult because I have coping strategies in place that I can ramp up or will it make it more difficult by compounding my existing difficulties? A couple of years into this grand hormonal adventure, I feel like it might be a combination of the two. Continue reading Autism and Menopause: More Questions Than Answers→
Catastrophizing is one of those autistic traits that when I first read about it, I thought, “Oh, I never do that.”
How wrong I was.
I catastrophize daily. It’s usually small stuff that blows over quickly–I’m not going to get to the post office before it closes which means I won’t get my important overnight package and I’ll have to go back tomorrow and everything will be delayed and I should have left home sooner and why did I take a right out of the parking garage instead of a left because taking a right always means waiting in more traffic even though it’s more direct well obviously it’s because I’m stupid and don’t think things through so it’s my fault if I get there too late but maybe I’ll be able to beg one of the workers who’s closing up to get my package because that worked once before and . . .
Next thing I know, I’m at the post office and it’s not closed. Crisis averted! Except this was a fake crisis, made up in my head because I was catastrophizing.
Snowballing a Crisis into a Catastrophe
I don’t mind minor catastrophizing. It’s annoying but not detrimental to my psyche like serious catastrophizing is. The serious type starts out small–like a case of poison ivy starts with just one little itchy bump–and gradually creeps up on me until I find myself taking a sledgehammer to my self-esteem. Continue reading Catastrophizing Sucks→
Let’s talk about interoception. I bet you’re already on the edge of your seat, right?
Okay, okay, first a definition. Interoception describes our sensitivity to sensations that originate in our bodies. Think pain, temperature, itch, sensual touch, sensations from our organs and muscles, hunger, thirst, and breathlessness.
All of these sensations combine to give us a sense of sentience. I’m hungry therefore I am.
Our Body’s Dashboard
Interoceptive feedback is important for keeping our bodies in good working condition. Think of them as the body’s dashboard. Are we low on fuel? Running too hot? Has it been too long since some critical service was performed or is a warning light flashing? Interoceptive sensations provide the feedback necessary for troubleshooting and correcting imbalances in the body.
Emotions often arise from our interoceptive sensations, too. When someone asks how you feel, you probably subconsciously check-in with your body, and realizing that you’re tired, hungry, hot, or achy, you reply, “not too great.” Or conversely, if your interoceptive sensations are in balance, you might report feeling happy or at least content.
Obviously not all emotions are tied to interoception, but it’s hard to be happy when you’re in pain or content when you’re itchy. For many people being hungry or tired is a direct route to being cranky and short-tempered. Those of us who are alexithymic experience this even more strongly, often struggling to identify the difference between emotions and physical sensations. I can’t explain how my body confuses “upset” with “cold,” but sometimes it does. Now I know that if I’m feeling cold when no one else around me is, I need to check in with my emotions. And put on a hoodie.
Engage Interoceptive Dampeners
But what if your interoceptive system is dampened? What if a sensation needs to be in the red zone before it comes up on the dashboard? Well, then you forget to eat or stare in wonder at your bleeding toes or don’t realize you might be in pain until you pass out. Sound familiar?
Many autistic people have dampened or muted interoception. We just don’t seem to notice what’s going on in our bodies until it reaches a level that other people would find intolerable. And often when we do notice it, it goes from “oh that’s happening” to intolerable really darn fast.
As often as I experience this in minor, inconvenient ways, I’m occasionally reminded of how dangerous it can be. Because hindsight is 20/20, I can see in retrospect that I recently had a UTI coming on for days before I picked up on the symptoms. One of the main symptoms is pain and other than a vague crampy feeling, I wasn’t experiencing any. Easy to ignore, so I did.
Then some harder to ignore symptoms started happening and my daughter, who I was visiting at the time, said, “you need to go get this checked now.” Left to my own devices, I probably would have taken a wait-and-see approach which would have been bad. Because a few hours later, shortly after getting my prescriptions filled, I was in intense pain. An hour early, at the walk-in clinic, the doctor asked me if I had any pain and, after thinking about it for a moment, I said, “maybe a little?”
My body had gone from zero to “MAKE IT STOP” in less than hour.
And thanks to my body’s poor interoceptive workings, I was rewarded with a kidney infection because unlike most women who dash off to the doctor at those first signs of a UTI, I wasn’t getting enough data to trigger my internal alarms. It wasn’t until I started having more obvious symptoms that I realized something might be wrong and took to Google to figure out what it could be. By the time I started getting the right antibiotics in my body, a common minor ailment has progressed to a potentially serious illness that I’m just starting to recover from two weeks later.
Unreliable Indicators
One of the purposes of interoception is to drive behavior.
Hungry? Eat.
Tired? Sleep.
Pain? Seek help.
Interoceptive sensations–especially pain–may be unreliable indicators in autistic individuals. Medical professionals often rely on pain and other self-reported symptoms of discomfort to assess the presence or seriousness of an illness. In my case, my interoceptive sensations were saying “meh” but my fever (which I didn’t realize I had) and high bacterial count were saying, “hey, big problem here!”
When you combine muted interoception with poor executive function–which may be further impaired by the stress of illness–you’ve got a recipe for disaster. This is why I need someone else to say, “we’re going to the doctor now.” It’s also why recognizing that autistic people may have unique pain, distress or illness signals is important for medical professionals, caregivers and loved ones. This can potentially lead to misdiagnosis or underdiagnosis.
Our nonstandard brain wiring can mean that we miss common warning signs or have difficulty knowing when to act on distress signals.
I’ve slightly revised the schedule due to some additional questions that were posted over the weekend. This week we’ll do general coping strategies. Next week we’ll do special skills and fun stuff. When I get back from my great big adventure some time in May, we’ll do acceptance and gender/sexuality/body image.
You all probably know the drill by now, but in case anyone new wanders in: answer as many questions as you like, here or anonymously at Survey Monkey. Talk amongst yourselves about the answers if you like.
Although some questions reference diagnosis, this is open to all those who identify as on the spectrum (professionally diagnosed, self-diagnosed and suspected aspies/autistics/people with autism).
General Coping Strategies
What positive changes did you make to your life after your diagnosis?
Over-apologising/apologising as a reflex action: Seriously, “sorry” has become my standard greeting to people at uni. Does anyone else do this? Has anyone managed to break the habit? How?
How do you all describe what it’s like to be you to someone else? What do you compare these things to in a way that makes others have that aha! moment? more details here
Does anyone else have issues with conflict/arguments/shouting matches in front of you? How do you deal with this?
How do you stay on top of cleaning? What contextual cues do you use to get you to do things around the house?
Do you catastrophise and if so, have you strategies for managing it?
Do you experience emotional distress, such as depression and grieving, in unusual ways, such as increased sensory challenges or physical pain?
Do you have trouble speaking at a normal pace? Do you have any tips for modulating your voice?
Have you experienced chronic fatigue or chronic pain? Do you have other chronic illnesses? If so, do you think autistic traits such as poor emotional awareness and sensory differences such as oversensitivity to pain or muscle discomfort have any effect on these?
This week for Take-a-Test Tuesday I took the Cambridge Mindreading Face-Voice Battery (CAM) which is another test of the ability to recognize emotions in others.
The Cambridge Mindreading Face-Voice Battery (CAM) tests recognition of complex emotional states. It consists of short audio and video clips in which actors convey 1 of 20 different complex emotions through either their voice or their facial expressions.
The theory behind the CAM is that autistic people are able to read basic emotions but have difficulty interpreting complex emotions. Basic emotions are the ones that we learn early in life: happy, sad, angry, surprised. Most people learn these by age 6.
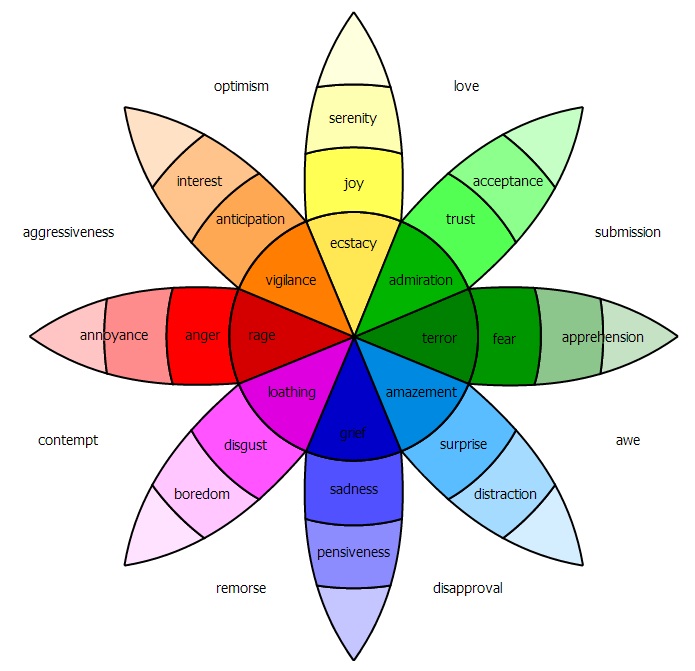
Complex emotions are sometimes described as combinations of basic emotions or as basic emotions plus cultural conditioning. They include mental states like stern, intimate, guarded, admiring, submissive and vibrant. There are hundreds of complex emotions and it takes us years to learn them. Generally, most people can recognize the majority of complex emotions by the time they reach adulthood.
Robert Plutchik’s Wheel of Emotions is one of many ways of thinking about the relationships between basic and complex emotions
According to the CAM creators, the emotional states presented in the clips are “higher order” emotional concepts:
6 concepts from level 4 (concepts understood by typical 15–16 year olds)
13 concepts from level 5 (understood by typical 17–18 year olds)
1 concept from level 6 (words understood by less than 75% of typical 17–18 year olds)
The purpose of the test is to examine whether autistic people grasp these more complex emotional states. It includes both negative and positive emotions as well as subtle and intense emotional states. Each of the 20 emotions is repeated 5 times.
Taking the Test
The Face-Voice Battery has two parts. Part 1 consists of listening to 50 short clips of actors saying a phrase or sentence. You’re given 4 options for describing the emotional content of the clip. Part 2 consists of watching 50 3-5 second videos of actors silently portraying facial expressions. Again you’re given 4 options that describe the emotional content.
You can take the Cambridge Mindreading (CAM) Face-Voice Battery at aspietests.org. To begin, click on the The Cambridge Mindreading Face-Voice Battery – Part 1 (Voices) link. After entering your age and diagnostic status and accepting the terms, you can proceed to the voice clips. As you take the test, keep in mind that speed counts. In addition to a %-correct score, the test returns an “average time to answer” score. Part 1 took me about 10 minutes to complete.
Once you finish Part 1, click the “back to the homepage” link and then click the Cambridge Mindreading Face-Voice Battery – Part 2 (Faces) link to begin Part 2. Again, speed counts. This part took me about 10 minutes to complete as well.
Scoring the Test
I did well on this test–in fact, I matched the mean score of neurotypical females in the original research study. Here is my score:
You scored 90.0% in 5.7 seconds. Faces: 84.0% (42 correct) Voices: 96.0% (48 correct)
NT Faces task: 44 correct (88%)
NT Voice task: 43 correct (86%)
NT Total: 86 correct (86%)
I’m not surprised by how well I did on the voices portion of the test. “Voice data” is my primary means of reading social situations. It helped that the informational content of the phrases matched the emotional content of the voices. For example, when I heard “that is horrible” I took into account the information being conveyed by the statement as well as the tone of voice to settle on my choice of “appalled.” This is considered a “strategy” by the test creators, so basically, once again, I’m “cheating.” But it works, so hooray for adaptations.
The video clips were a mixed bag. I think I did better on the ones that had a dissimilar set of possible answers (i.e. appalled, vibrant, blank, or intimate) and the ones that I remembered to glance at the answer choices before the clip played.
As an experiment, for some trials I watched the clip and tried to form an answer before looking at the choices. On one video, I was certain the answer was “sarcastic” but that wasn’t one of the choices; I think the correct answer was “reassured.”
A few other random thoughts:
Am I the only one who thought most of the voice clips sounded like they were straight out of Dickens novel?
The use of live action videos is more realistic than static photos, but I still didn’t feel like the test results were reflective of my real life ability to read emotions.
I liked seeing the contrast in my voice vs. facial expression reading skills.
Some of the video clips made me incredibly uncomfortable to the point that I had to glance away.
I couldn’t find any data on the “time to answer” scores. From background reading about this type of test, I know that researchers often use the average time to answer as a metric to gauge competency. The assumption is that the longer it takes to answer, the more processing your brain is doing to produce an answer.
The Bottom Line
CAM feels more realistic than Reading the Mind in the Eyes, but it’s still far from an accurate test of the fluid way that emotions present in real life interactions.
This week for Take-a-Test Tuesday we’re taking the online alexithymia questionnaire.
Alexithymia refers to people who have difficulty identifying and describing emotions as well as differentiating between physical and emotional sensations. It’s not a formal diagnosis, but a way of describing a common set of experiences related to emotional dysfunction.
Some descriptions of alexithymia also include impoverished imagination and a tendency toward externally oriented (concrete) thinking. I found it interesting that both studies I cite below omitted these last two characteristics. Many of you who commented on the emotional dysfunction post last week questioned the inclusion of impoverished imagination, saying that you personally felt the opposite was true. I have to agree with this. My imagination is, if anything, overactive. Perhaps there is an autistic subtype of alexithymia?
Alexithymia is extremely common in autistic individuals. About 50% of people diagnosed with ASD have severe alexithymia, however nearly all people on the spectrum experience it to some degree. Among the general population, about 10% fit the alexithymia profile and parents of autistic children are more likely to be alexithymic than parents of nonautistic children.
When it comes to social communication, the line between autistic traits and alexithymic traits is blurry. Two recent studies (Bird et al, 2010 and Silani et al, 2008) suggest that alexithymia, not ASD, is responsible for impaired affective empathy.
The 2008 study looked at brain activity in autistic and nonautistic people with and without alexithymia. It found a correlation between a person’s level of alexithymia, brain activity in one of the regions believed to be responsible for identifying one’s own emotions, and scores on an empathy questionnaire. This was true of both the autistic and nonautistic participants, suggesting that impaired processing of emotion, not autism, is the source of impaired affective empathy.
The brain uses the same neural pathways for perceiving and interpreting our own emotions as well as the emotions of others, so it makes sense that if we cannot process our emotions easily, we’ll also struggle to process emotions demonstrated by others..
One question that remains unanswered is why autism and alexithymia occur together so frequently.
Many commenters on last week’s post recognized themselves in my description of my own emotional dysfunction, so I thought it would be interesting to take the Online Alexithymia Questionnaire. While not a clinically recognized measure of alexithymia, it is based on commonly used clinical screening questionnaires.
Pros and Cons of the Online Alexithymia Questionnaire
Pros
Self-scoring
Provides subscale scores with cutoffs
Overall score is presented on a simple visual “severity” scale
Includes questions phrased as self-observation (I feel . . .) and other observation (People tell me . . .)
Cons
Not clinically tested or validated
Unclear how cutoffs were derived
Includes questions on topics that are not a part of generally accepted alexithymia definition
Taking the Test
The alexithymia questionnaires used in clinical research (TAS-20, BVAQ) aren’t available online, so I took the Online Alexithymia Questionnaire (OAQ-G2).
Take the test here. There are 37 questions. You have to answer at least 20 to get a result, meaning you can skip any you find overly invasive. The answers for each question become “grayed out” once you make a selection but you can go back and change your answer if you want to.
Scoring the Test
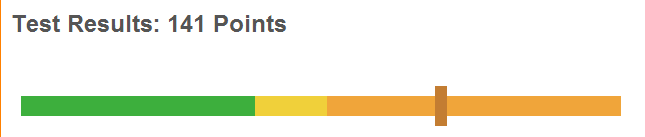
When you’re satisfied with your answers, click the “Evaluate Test” button and you’ll be given an overall score as well as 7 subscale scores. Here are mine:
Test Results: 141 Points. Alexithymia: You show high alexithymic traits.
The yellow area indicates “some alexithymic traits” and the orange area indicates “high alexithymic traits”
Sexual Difficulties and Disinterest: 11 Points <10 – 12> some alexithymic traits
The subscale scores in parentheses appear to be equivalent to the yellow area on the slider bar, meaning “some alexithymic traits.” A score below the range in parentheses indicates the absence of alexithymic traits (green area) and a score above indicates high alexithymic traits (orange area).
Keep in mind that the last two subscales, problematic interpersonal relationships and sexual difficulties/disinterest, aren’t specifically part of the formal definition of alexithymia. It’s possible that the sexual difficulties subscale could be impacted by whether a person is in a long-term relationship and feels comfortable with their partner. Also, externally-oriented thinking and restricted imaginative processes are not always included in clinical definitions of alexithymia. The first three subscales are the best gauge of the core deficits of alexithymia.
I was surprised by my score on externally oriented thinking. This item refers to a tendency to think in concrete, nonintrospective terms. I don’t view concrete and nonintrospective as synonymous, but that could be my autistic brain.
I think in concrete terms, but I also spend a lot of time examining my thoughts and feelings. I might spend more time on the latter because I have to consciously “check-in” with my feelings to identify them. However, neurotypical people may be spending more time considering their feelings as part of decision making or social interaction. My introspection usually tends toward “what the heck is going on?”
The Bottom Line
The Online Alexithymia Questionnaire is the only freely available alexithymia test. Although not scientifically validated, it appears to be a reasonable “amatuer” measure of alexithymic traits and a useful starting point for better understanding how you process emotions.
NT: Fine. Don’t tell me. I was just trying to help.
When an aspie says they don’t know what they’re feeling, it’s a literal statement. We aren’t trying to dodge the conversation. We aren’t withholding information. We aren’t being rude, mean, cold coy or vindictive.
I’ve had variations on the above conversation many times and it’s as frustrating for me as it is for the person who wants to know what’s wrong. The reason? I have difficulty identifying my emotions and even more trouble verbalizing them. Working through my emotional constellations has helped me identify some of the specific issues I–and many autistic people–have in processing and identifying feelings.
(Photo: Joe Shlabotnik / Creative Commons)
Predictably, I’ve grouped the issues into three general categories:
modulation (moderating the strength of my own emotions)
determination (identifying emotions in others)
discrimination (separating emotion directed at me from general expression of emotion)
Modulation: The Glitchy Volume Control
There is a common misconception that autistic people are unemotional. You’ll often hear this refuted by autistics themselves, who say they are too emotional. So which is it? For me, it’s both. My emotions gravitate toward the extremes of muted or intense; few emotional experiences fall in the midranges.
My default emotional state is neutral. I don’t feel especially good or bad. I’m present in the moment and content to be so. Externally, I may come across as serious or subdued, but reduced expressiveness shouldn’t be confused with a negative state of being or a lack of feeling.
The feelings are definitely there. Most of the time they quietly mind their own business and I need to consciously check-in to see what they’re up to. When they decide to fully surface on their own, however, they’re intense.
Unlike most neurotypicals, I don’t have a lot of ability to modulate the strength of my emotions. Imagine a radio with an on/off switch and a glitchy volume control.
If you think about this in terms of the weak executive function associated with Asperger’s, it makes sense. Humans use reasoning, rationalization and labeling to modulate emotion. All of these methods fall under the umbrella of executive function. Labeling emotions, in particular, seems to be hard for aspies.
Determination: The Broken Mirror
Just as I have difficulty labeling my own emotions, I have trouble identifying what others are feeling. I struggle with interpreting facial expressions and body language. I’m weak at perspective-taking. Basically, when it comes to reading emotional clues, I’m like one of those old-time detectives who had to solve murders without any forensic evidence. There’s only so much information you can gather from what people tell you outright.
This difficulty determining what others are feeling is a big contributor to the stereotype of the empathy-deficient aspie. If someone is giving off “I’m sad” cues that I fail to recognize, when I don’t console them, they’ll assume I’m cold and unsympathetic.
For neurotypical people, emotional interaction is like looking in a mirror. They expect to see a reflective emotion looking back at them and when they don’t, they assume the mirror is broken.
This isn’t to say I’m oblivious to other people’s emotional states. I get the obvious ones and the ones that I can derive from contextual clues. What I tend to miss are the subtle or unexpected emotional states.
Discrimination: Missing the Target
I’ve always been disturbed by confrontation and conflict, even when I’m only a bystander. By default, The Scientist is in charge of “confrontation with others.” If something needs to be argued over or complained about–a botched repair job or an over-cooked restaurant meal–that’s his department. While he’s making that phone call or waiting for the manager to appear, I go off and hide.
As an adult, I’m not proud of this. Why do I desperately need to flee a situation to which I’m nothing more than an observer?
Because, I recently realized, I don’t discriminate between anger that is aimed at me and anger in general. When someone is angry, I invariably feel like I’m the cause or the target, even when I rationally know that I’m not.
If The Scientist calls me after a bad day, I hear how upset he is and immediately feel distressed. Not distressed as in “I should console my husband because he’s had a bad day.” I feel distressed in a “this is incredibly stressful and I want it to stop” kind of way. My brain immediately goes into “fix it” mode, searching for a way to make the other person feel better so I can also relieve my own distress.
Of course, a conversation with an upset spouse is upsetting to most people. But what about a conversation between two strangers that I’ve merely overheard? Twice in the past two weeks I’ve witnessed one person berating another for an etiquette infraction at the swimming pool. (Yes, we take our lap swimming seriously around these parts.) Both times I felt my heartbeat skyrocket, as if the anger was directed at me. In reality, I’m sure neither of these people even noticed I was standing nearby.
Even now, as I’m sitting here in Starbucks typing, the woman at the next table is telling a story about how mad she is at her sister-in-law; I can feel my blood pressure rising at the tone of her words. Words that are completely irrelevant to me. Words that, thanks to my funky brain wiring, I find impossible to tune out.
Yes, not only does my autistic brain not know how to interpret the emotional content of other people’s conversations, it also refuses to tune them out. And people wonder why we aspies like to spend a lot of time alone.
It took me a long time and a lot of thought to figure out why I respond to secondhand distress like this. Why should I feel emotionally assailed when the angry words are aimed at another person?
In part it’s related to my upbringing, but there is also an element of weak executive control at work. In theory, I should be able to rationalize away my overreaction by telling myself that I’m observing generalized anger (or frustration or sadness), not anger directed at me. I should be able to put myself in the other person’s shoes and direct my emotions at the target of their distress, rather than feeling like the target myself.
Alexithymia
The three areas where I have difficulty–modulation, discrimination and determination–are actually core traits of alexithymia.
Alexithymia (literally: having no words for emotions) is impairment in identifying and describing emotions. Specifically, it’s characterized by:
difficulty identifying feelings
difficulty distinguishing between feelings and bodily sensations related to emotional arousal
difficulty describing feelings to others
impoverished imagination and fantasy life
a stimulus-dependent, externally oriented cognitive style
When I look at the list of alexithymic characteristics, I also realize that when I’m emotionally uncomfortable, I’m more likely to have physical complaints. I’ll be feeling frustrated or sad, but complain that I’m uncomfortably cold or intolerably sleepy. This isn’t a connection I would make on my own, but once I see it described as part of alexithymia–like so much about my autistic self–it suddenly makes perfect sense.
There is a lot of overlap between alexithymia and ASD, both in the perception of emotions and the difficulty in verbalizing feelings. Not only are autistic people very likely to exhibit the characteristics of alexithymia, their parents are as well. However, many non-autistic people also have alexithymia, so it isn’t exclusive to ASD.
Alexithymia isn’t a clinical diagnosis like autism. It’s a construct (theory) used to describe the traits of people who have difficulty verbalizing emotions. It’s also a helpful way of thinking about some of the challenges that aspies have with processing feelings.
—–
More on Alexithymia and ASD:
Next Tuesday, we’ll be doing the Alexithymia Questionnaire for Take-a-Test Tuesday.
Alexithymia and Grief at Unstrange Mind is a challenging and insightful piece about the mourning process
Great example of an Alexithymia cheat sheet in the form of a flow chart at Radical Neurodivergence
Sadness feels like the emotion that is most strongly connected to humanity–the one that binds us to each other in some important and primitive way.
I can be happy by myself. I’m as likely to be angry with myself as with someone else. But sadness–I usually need another person to tip me over into feeling sad.
Like my anger constellation, my sadness constellation required a thesaurus. Once I got past grief, depression and resignation, I needed help identifying other types of sad feelings. But unlike my exploration of anger, the thesaurus wasn’t much help this time. I added a few more words to the constellation, but I’m not sure how strongly I experience any of them.
My sadness constellation, sketched out on a Starbucks napkin
Sadness feels like a diffuse emotion, more of a background state of being than a tangible feeling. I’m rarely “actively” sad. I don’t burst into tears when I hear sad news. The last time I cried at a movie, I was twelve. The only book that ever made me tear up was A Prayer for Owen Meany. More than once I’ve sat stoically immobile beside someone I love while they broke down.
My sadness is all undercurrent, twisted up inside me, unable to escape to the surface. This, of course, makes me look cold and unfeeling. The stereotypical cold-hearted aspie.
The first time I confronted my muted sadness was in high school. Junior year. A girl in my class, Karen, was killed in a car accident. The entire junior class attended her funeral, and everyone sobbed from beginning to end. Except me.
I remember standing there, my best friend crying against my shoulder, and feeling . . . confused. I barely knew Karen. She was one of the “fast” girls, part of a small clique that didn’t mix in with the rest of the class much. Many of the girls crying that day in church wouldn’t have hesitated to whisper something mean about Karen or her friends when she was alive. Yet here they were, brokenhearted. This made no sense to me.
Of course I felt sad that she’d died. It was a horrible tragedy. But obviously I didn’t feel as sad as everyone else. If I had, wouldn’t I be crying, too? Soon this thought consumed me. In desperation, I tried to make myself cry by thinking of sad things, by focusing on how sad this day was. I squeezed my eyes tightly closed until they started to water. A few teardrops fell but mostly what I felt was a sick, sinking panic.
While everyone was mourning the loss of our classmate, I alone was wondering: What’s wrong with me? And afterwards, while everyone was getting drunk to soothe their pain, I was hoping that if I got drunk enough, I’d somehow gain access to this mysterious thing called grief.
While I’ve experienced loss since then, my experience of grief is uneven and unpredictable. Sometimes my reaction to death is a sadness so strong and overpowering that it becomes physically painful. Other times I feel like my grief is strangled inside me with only the smallest of escape valves to trickle through. In this sense, grief frightens me. I feel like I haven’t practiced enough and when the big day comes, I’ll be unprepared, like a boxer entering a title match with only a few amateur bouts under her belt.
The rest of my experience with sadness is no less confusing. Most often sadness equals resignation, that sinking feeling that no matter what I do, the underlying characteristics of a relationship or a situation will never change. I used to be more of a fighter, wanting to fix everything and everyone, but increasingly I’m resigned to what is.
This is good and bad. Good because I’m relinquishing my intense need for control; bad because resigning myself to a situation can feel like giving up, and giving up can lead to hopelessness. I put a question mark next to hopelessness because it’s rare and transient. I’m an optimist at heart and if studying economics taught me anything it’s that in the long run, everything can change.
Sometimes I get the blahs. Life looks dull and unappealing. My natural enthusiasm evaporates and I’m left with a gray cast over everything. I’m not sure if the blahs have a specific trigger or if they’re hormonal/cyclical. I’ve seen other aspies talk about being unexpectedly overcome by a general feeling of sadness and not being able to identify the source, which is exactly what I associate with the blahs.
Fortunately, I have an emotional reset button. If I go to sleep feeling down, I’ll usually wake up the next day feeling fine. If I don’t reset overnight, the blahs can stretch into ennui. I’ll get bored and restless, lose my focus, bounce around between tasks accomplishing little or nothing. My routines break down, which only increases my restlessness and lack of focus.
At this point, I need to make a conscious effort to get myself back on track or I risk slipping into depression. A lot of aspies struggle with depression, either as a periodic state or as a clinically comorbid disorder.
My experience with depression has been the less severe, episodic type: a period of feeling down and discouraged, usually in response to something someone has done or said. But I’m mellowing with age, each passing year lessening my need to beat up on myself in response to other people’s slights and judgments. These days I’m more likely to chuck unpleasant interactions into the resignation bin and move on.
That leaves only distress. Is distress really a form of sadness? Some of the synonyms I found for it certainly are: agony, misery, suffering, anguish, torment. I’ve always associated distress more with anxiety or fear, but thinking about it now, I do sometimes feel distress as a form of sadness. I have a fear of abandonment and that fear can trigger a deep-seated, overwhelming distress.
Asperger’s is such a paradoxical condition. I love being alone but I fear abandonment. I don’t often experience unmitigated grief but when I do, it’s overwhelming. I need a thesaurus to help me identify the shape of my feelings, but once I put names to them, they come alive for me in very specific ways.
If you look at my constellation, you’ll see that I added regret and melancholy but after some reflection I put an X next to them. I don’t spend a lot of time looking backward, especially not in a sad way. I’m more of a “learn from it and move on” kind of person. The present moment is more alive for me than any ghost of a memory.
Since learning more about Asperger’s I’ve come to wonder if my muted sadness is a self-protection mechanism. When I wrote about happiness and anger, I talked about the unfiltered versions of these emotions that I experience–the emotions that feel particularly autistic in nature.
I’m far less equipped to handle unfiltered sadness. When it comes, it’s crushing. I think my subconscious instinct is to mute the intensity. There is, after all, only so much sadness a person can handle. So I experience sadness in my own way, inwardly, quietly.
The Purpose of Sadness
I read recently that the “evolutionary purpose” of sadness might be to trigger reflection after a major life event. When we experience loss or a setback, it makes sense for us to withdraw and reevaluate our lives. The result is often a life-changing insight or decision.
If this is the case, my sadness serves me well. I turn inward, often and intensely, searching for answers, insight, a truer path. Even at that funeral in high school, in the absence of grief, I was looking inward. Sad, perhaps, in a very similar way to the rest of the girls, though I didn’t understand it then.
As an adult, I know that the teenaged girls in that church were mourning more than the loss of a classmate. They were mourning the loss of their own innocence. They were confronting the cruelty of life. They were facing the dangers that adulthood holds, the possibility that it could have been any one of us rocketing down the highway one moment, dead at the bottom of a cliff the next.
They were sad for Karen, sad for themselves, frightened, overwhelmed. When I look at it in that context, I see that my feelings weren’t that different from theirs. I struggled with the expression of my sadness–I still do–but it’s been there all along.