These past few weeks I’ve had a sensory comfort zone the size of a postage stamp. There are a few things playing into my increase in sensory sensitivities* and one of them is definitely the change of seasons. Transitioning from summer to winter or vice versa is surprisingly demanding.
I think the biggest factor is the constant sensory adaptation. During the winter and summer, the days are pretty consistent from one to the next. It might be uncomfortably hot or cold, but at least my body knows what to expect each day and dressing appropriately doesn’t require a lot of forethought.
Spring and fall, on the other hand, are filled with unpredictable days. Yesterday was t-shirt weather. Today I have on sweats and a thermal shirt. Three days ago I left all of the windows open overnight because it was uncomfortably warm in the house. This morning I dashed out of bed to close the kitchen window, which was open two inches and letting a cold draft in.
With each temperature fluctuation, I find my body struggling to adapt. Too hot. Too cold. Over dressed. Underdressed. It’s hard to find that sweet spot–a consistent, comfortable environmental and body temperature. For the average person, this probably isn’t a big deal. I imagine things like dressing in layers and putting on or taking off clothing as needed is a good solution.
The problem with that strategy is that thanks to wonky interoception I often don’t notice when I’m too hot or too cold until it reaches a level of mild to moderate physical distress. At that point, doing something about it requires not just taking off or putting on a layer, but lowering or raising my body temperature to a comfortable level again. Simply putting on a sweater isn’t a complete solution to whole-body shivering. Continue reading Changing Seasons and Sensory Sensitivities→
This is the final part in a series about sensory sensitivities and atypical sensory processing. Read the other parts: Part 1 | Part 2 | Part 3
When we think of diet or dieting, we usually think of restricting our intake in some way. But a sensory diet isn’t about restriction, it’s about fulfilling sensory needs and improving self-regulation with a specific selection of sensory activities.
The term sensory diet originated in the occupational therapy field and is commonly used in relation to both autism and sensory processing disorder. To create a sensory diet, an occupational therapist looks at a person’s areas of sensory hypo- and hyper-reactivity and comes up with ways to help up-regulate or down-regulate them.
This video has some great examples of the types of sensory activities that are often prescribed:
Going Up?
Sensory diet activities come in two flavors: upregulating and downregulating. Upregulating activities help to stimulate under-reactive senses. Downregulating activities, in contrast, help calm over-reactive senses.
Sometimes an activity that is upregulating for one person or in one situation can be downregulating for another person or in a different situation. For example, bouncing on a trampoline can stimulate the proprioceptive sensory channel but it can also help calm someone who is overloaded (by releasing excess energy). Continue reading Sensory Diet→
This is part 3 in a series about sensory sensitivities and atypical sensory processing. Read the other parts: Part 1 | Part 2 | Part 4
——-
While atypical sensory filtering is related to sensory sensitivities, not all unfiltered sensory data will trigger sensitivities. Remember the sounds I described hearing as I’m typing this? I’m not especially sensitive to any of them. I hear them and it’s hard to tune them out, but I don’t have a biological stress reaction to them. They’re just there and over the years I’ve grown used to having a lot of irrelevant aural data constantly pinging around in my brain.
In fact, I didn’t know until a couple of years ago that other people don’t hear all of those distinct ambient sounds when they’re engaged in an activity.
I suppose what’s happening in this case is my sensory gating is failing, letting the irrelevant sounds in. They get routed to an area of my brain that says, “oh, right, traffic, dog, sirens, rain, typing, closer traffic, harder rain, actually two dogs, footsteps upstairs” and on and on.
What should happen when I hear those repetitive background noises is something called habituation. The first time the dog down the hall barks, my filtering system might kick it upstairs to my decision making brain and say, “hey boss, is this something we need to worry about?” The decision making region would analyze the situation, decide that the dog is neither a threat nor any of my business, and say, “nope, ignore that from now on.” The filtering system would then flag that gate for closing, eventually tuning out the repetitive barking until I stopped noticing it.
This is part 2 in a series about sensory sensitivities and atypical sensory processing. Read the other parts: Part 1 | Part 3 | Part 4
——
I don’t like pistachios.
I have a sensory sensitivity to bright lights in a dark room.
What’s the difference between the two? I can eat pistachios if I have to. I won’t enjoy it, but if I happened to be served something that had some pistachios on or in it, I could eat it without having a negative biological reaction.
On the other hand, I can’t watch TV or look at a computer monitor in a dark room. The brightness of the screen is painful and my instinctive reaction is to look away or close my eyes. If The Scientist and I are watching TV at night, I need a small amount of ambient light to reduce the contrast between the television screen and the darkened room. Without it, I’ll squint at the screen and quickly develop a headache.
I know this because, like the t-shirt incident, I’ve tried to acclimate myself to watching TV in the dark.
I can see how someone who doesn’t know that I have sensory sensitivities might assume that I dislike watching TV in the dark in the same way that I dislike pistachios. If you’ve never experienced sensory sensitivities, it can be hard to believe that they’re real and that they have a biological component to them. But my body’s reaction to those two scenarios is very different. Continue reading The Difference Between a Sensory Sensitivity and Disliking Something→
This is the first in a series of posts about autistic sensory processing and sensory sensitivities. Part 2 | Part 3 | Part 4
—–
I once had a t-shirt that I really wanted to like. It was a souvenir from a trip to Hawaii. The color, the material, the fit, the design–all perfect. It would have been my favorite new shirt, except for one thing.
It had a tiny thread in the collar that scratched my neck. A thread so small that I couldn’t see it. I’d cut out the offending tag and all of the visible stitching holding the tag in place, but that one little thread refused to go.
So I decided that I was going to get used to it. I was going to pretend that evil remnant of plastic thread didn’t exist. If it was too small to see, surely I could ignore it.
I tried. I really did.
I put the shirt into my summer t-shirt rotation and wore it at least once a week. The material got softer with each washing, which only made me want to love it more. It was one of the most comfortable shirts I owned. It would have been that most elusive of things–the perfect shirt–except for that microscopic thread.
I developed seriously mixed feelings about the shirt. I was determined not to let the thread win. It became A Thing. Some days I would wear it all day, doggedly ignoring how the thread jabbed at the back of my neck when I moved this way or that way. Other days I’d only make it to early afternoon before tossing the shirt in the laundry and changing–with a sigh of relief–into a more comfortable shirt. One with the tag cut cleanly out.
This went on for years. I wore the shirt in spite of how it made my neck itch and burn, in spite of the way it made me unconsciously pull at my collar all day long. I wore it right up until the day I admitted to myself that I was never going to get used to that thread. Putting my Hawaii shirt in the donation bag felt like a defeat. A thread–so small it was invisible–had gotten the better of me. Continue reading Sensory Sensitivities and Atypical Sensory Processing→
I think I was born to be in motion. I have difficulty resting when I’m at rest.
If I have to sit in one place long enough, I’ll cycle through dozens of postures without thinking about it. I slouch. I splay. I pin one foot under the other. I pull one knee up, then two, hugging my shins with a hand or arm. I sit on my foot, ankle or calf. I sit crossed legged, even on chairs. I put my elbows on the table, lean my head or chin on my hand, interlace my hands on top of my head. I perch on the edge of my chair, turn sideways, tangle my feet in the legs of nearby furniture.
The variations are endless but they have one thing in common–they orient my body to my surroundings. Without a steady stream of proprioceptive feedback, I start to feel disoriented and disconnected from my body. I feel lost in space. Confused. Physically disorganized..
When I’m at home, sometimes I just go lie on the floor to give my body a break from being upright. Because being upright requires figuring out where to put my hands and arms and legs and feet and often no sooner do I get that all sorted out than that restless feeling starts nudging at my leg or foot or spine and I need to move again.
It’s not that I can’t sit like a proper adult. I often start out sitting with both feet on the ground, arms relaxed at my side. In fact, in new social situations, I make a conscious effort to sit properly. Because I’m not four years old. I’m an adult–often an adult in a situation where I’m expected to look professional–and adults have very specific expectations of other adults in those situations.
Often what I come up with is a tense variation of typical “good sitting posture”:
Then my internal clock starts ticking and one of two things happens. If I’m in a formal setting, my body will grow more and more tense as I work to maintain a polite, socially acceptable posture. Then I’ll start covertly stimming, rubbing something between my fingers or twisting my hand in my pantsleg, something to counterbalance the tension that’s building up as I force myself to be still.
If I’m in comfortable or casual surroundings, it doesn’t take more than five minutes for me to start shifting around, searching for a more comfortable position. On an airplane, for example, I’ll start out sitting with my feet on the floor, book in my hand, arms close to my sides–typical polite seatmate posture. Soon, I’ll have one leg splayed out along the aisle or tucked under my opposite thigh. When that stops working, I’ll slouch and pin both knees against the seat in front of me or turn sideways and pull my legs up to my chest or fold one leg across the knee of the other, wedging a foot against the seat in front of me.
The fact that I’ll start stimming when I can’t freely change my posture often probably indicates that the positions I use to feel comfortable are in fact themselves a form of stimming.
Reset, Relax, Repeat
My body has a time limit on any one position. Even when I’m trying to fall asleep, if I don’t nod off right away, I need to keep changing position every ten minutes or so.
When I’m still, I have a gradual build-up of . . . I don’t know what. Tension? Discomfort? Disorganization?
I start to feel more and more uncomfortable until I have an uncontrollable urge to rearrange myself. Once I move into a new position, I’ll feel comfortable–momentarily at rest. Then, gradually, the discomfort starts building and soon I have to move again. Sometimes it’s only a matter of shifting back and forth repeatedly between two positions–a trick I used a lot at university to avoid adopting too many odd slouchy postures in class.
As important as the movement–and here’s where I think the particularly autistic aspect of this comes into play–is the position of my limbs. I almost always have one part of my body pinned, pressed, squeezed or wedged against or under something–either another body part or a piece of furniture. I think this deliberate pressure creates feedback that grounds me physically. It reminds me of where my body is in space and makes me feel safe in a way I can’t describe with words.
Physically, pressure equals organization.
Perhaps it’s like swaddling a baby. Mothers have been snugly wrapping up fussy infants for centuries. There is some science to back up the practice, suggesting that swaddling calms babies by enhancing motor organization and self-regulation. Once babies reach a few months old, swaddling is no longer beneficial or necessary because they have a reduced startle reflex and better-developed motor control.
Maybe there’s something very primitively calming about the kind of pressure I’m constantly seeking–a sort of localized form of swaddling.
Or perhaps it’s simply about feedback. Given my poor sense of interoception and my strong drive for proprioceptive sensory input, it’s not surprising that I need to intentionally create a steady stream of input to remind me that I physically exist.
Let’s talk about interoception. I bet you’re already on the edge of your seat, right?
Okay, okay, first a definition. Interoception describes our sensitivity to sensations that originate in our bodies. Think pain, temperature, itch, sensual touch, sensations from our organs and muscles, hunger, thirst, and breathlessness.
All of these sensations combine to give us a sense of sentience. I’m hungry therefore I am.
Our Body’s Dashboard
Interoceptive feedback is important for keeping our bodies in good working condition. Think of them as the body’s dashboard. Are we low on fuel? Running too hot? Has it been too long since some critical service was performed or is a warning light flashing? Interoceptive sensations provide the feedback necessary for troubleshooting and correcting imbalances in the body.
Emotions often arise from our interoceptive sensations, too. When someone asks how you feel, you probably subconsciously check-in with your body, and realizing that you’re tired, hungry, hot, or achy, you reply, “not too great.” Or conversely, if your interoceptive sensations are in balance, you might report feeling happy or at least content.
Obviously not all emotions are tied to interoception, but it’s hard to be happy when you’re in pain or content when you’re itchy. For many people being hungry or tired is a direct route to being cranky and short-tempered. Those of us who are alexithymic experience this even more strongly, often struggling to identify the difference between emotions and physical sensations. I can’t explain how my body confuses “upset” with “cold,” but sometimes it does. Now I know that if I’m feeling cold when no one else around me is, I need to check in with my emotions. And put on a hoodie.
Engage Interoceptive Dampeners
But what if your interoceptive system is dampened? What if a sensation needs to be in the red zone before it comes up on the dashboard? Well, then you forget to eat or stare in wonder at your bleeding toes or don’t realize you might be in pain until you pass out. Sound familiar?
Many autistic people have dampened or muted interoception. We just don’t seem to notice what’s going on in our bodies until it reaches a level that other people would find intolerable. And often when we do notice it, it goes from “oh that’s happening” to intolerable really darn fast.
As often as I experience this in minor, inconvenient ways, I’m occasionally reminded of how dangerous it can be. Because hindsight is 20/20, I can see in retrospect that I recently had a UTI coming on for days before I picked up on the symptoms. One of the main symptoms is pain and other than a vague crampy feeling, I wasn’t experiencing any. Easy to ignore, so I did.
Then some harder to ignore symptoms started happening and my daughter, who I was visiting at the time, said, “you need to go get this checked now.” Left to my own devices, I probably would have taken a wait-and-see approach which would have been bad. Because a few hours later, shortly after getting my prescriptions filled, I was in intense pain. An hour early, at the walk-in clinic, the doctor asked me if I had any pain and, after thinking about it for a moment, I said, “maybe a little?”
My body had gone from zero to “MAKE IT STOP” in less than hour.
And thanks to my body’s poor interoceptive workings, I was rewarded with a kidney infection because unlike most women who dash off to the doctor at those first signs of a UTI, I wasn’t getting enough data to trigger my internal alarms. It wasn’t until I started having more obvious symptoms that I realized something might be wrong and took to Google to figure out what it could be. By the time I started getting the right antibiotics in my body, a common minor ailment has progressed to a potentially serious illness that I’m just starting to recover from two weeks later.
Unreliable Indicators
One of the purposes of interoception is to drive behavior.
Hungry? Eat.
Tired? Sleep.
Pain? Seek help.
Interoceptive sensations–especially pain–may be unreliable indicators in autistic individuals. Medical professionals often rely on pain and other self-reported symptoms of discomfort to assess the presence or seriousness of an illness. In my case, my interoceptive sensations were saying “meh” but my fever (which I didn’t realize I had) and high bacterial count were saying, “hey, big problem here!”
When you combine muted interoception with poor executive function–which may be further impaired by the stress of illness–you’ve got a recipe for disaster. This is why I need someone else to say, “we’re going to the doctor now.” It’s also why recognizing that autistic people may have unique pain, distress or illness signals is important for medical professionals, caregivers and loved ones. This can potentially lead to misdiagnosis or underdiagnosis.
Our nonstandard brain wiring can mean that we miss common warning signs or have difficulty knowing when to act on distress signals.
The summer before seventh grade I went to an amusement park with my cousins. Until that day, my amusement park experience had been limited to kiddie rides. My parents weren’t roller-coaster-riding types and I guess they assumed I wasn’t either.
So there I was, first time in a real amusement park with real rides and roller coasters and everything and I was . . . terrified. I felt sick to my stomach just looking at the rides. But my cousins, who had been to the park many times, grabbed my hands and made a beeline straight for a ride that looked like this:
It was called Strawberry Fields and as we waited for it to start, songs from “Sgt. Pepper’s Lonely Heart’s Club Band” blared from the speakers overhead. My memory of that moment is clear as if it happened yesterday. I can hear the scratchy version of “Lucy in the Sky with Diamonds”, feel the greasy vinyl of the safety bar beneath my sweaty palms and practically taste my fear as my heart galloped in my chest.
And then we started to move, slowly at first, gaining speed, a little more and a little more until the wind was whipping my hair across my face and the three of us were pressed in a bone-crunching heap against the outside of the car and I was screaming right along with everyone else through 90 seconds of pure, unadulterated joy.
When the ride stopped all I could think was, “holy shit, let’s do that again!” And again and again and again.
I’d discovered one of my favorite sensory experiences: going fast. Blindingly fast. Mind-numbingly fast. The speed was exhilarating. I rode everything in the park. The faster it went, the more I liked it. Spinning, falling, dipping, swinging–I had no idea why I liked the intense physical sensations that the rides created, but I did. When I went back to the park on a seventh grade field trip, I spent the morning riding a roller coaster, jumping off and running around to the entrance to get right back in line.
Sensory Seeking =/= Stimming?
Now that I know about sensory seeking behavior, my sudden intense love of amusement park rides makes sense. Autistic people are often sensory seeking in a big way. We have a strong need for intense sensory input and will deliberately seek out or create sensory experiences to satisfy that need.
Sensory seeking is often described as a way to either stimulate an understimulated nervous system or calm an overstimulated system. Which sounds a lot like the typical definition of autistic stimming.
That raises the question: is sensory seeking behavior a form of stimming? There is a lot of overlap between the two, but I don’t think they’re identical. Stimming provides sensory input so I think we can say that all stimming is sensory seeking. But stimming is generally repetitive, which isn’t always true of sensory seeking.
Going on a roller coaster once or twice? Probably sensory seeking. Going on a roller coaster twenty times in a row? Could be stimming.
Honestly, I have no idea. Feel free to weigh in with your own theory, opinion or confusion in the comments.
The Wild Ones
Much of my childhood play was sensory seeking in disguise. Some of my favorite activities as a kid:
Going as fast as I could down big hills on my bike, roller skates or sled
Jumping or diving off the high board
Hanging upside down and doing somersaults on the monkey bars
Jumping on the bed (broke my jaw doing this)
Bouncing on a trampoline or Hippity Hop
Sit ‘n spin!
Climbing trees and hanging upside down from the branches or jumping to the ground
Running into the padded gymnasium wall and bouncing off
Zipping my arms into my coat and playing crash dummies with a friend (this never ended welll)
Lying underneath my beanbag chair while watching TV
Swinging as high as I could on the swings then flying off
These are not especially “girly” pastimes. They’ll get you branded a tomboy and a handful. If you’re a boy, you’ll be seen as wild and unruly, maybe you’ll get an ADHD diagnosis.
My next door neighbor had a Hippity Hop and Sit ‘n Spin–neither of which my parents would buy me. I didn’t especially like my neighbor but I loved her toys.
As a teenager I took up martial arts, primarily for the self-defense aspect of it, but I discovered that I liked the contact that sparring involves. Getting hit while padded up with gear creates a very tangible kind of physical feedback. So does pounding a heavy bag or kicking a hand target hundreds of times in a row.
Although that may sound masochistic, it’s not. I don’t seek out pain. Let’s be clear about that. Although I often engage in activities that have a risk of injury and pain, what I’m looking for is a benign physical sensation–one of pressure or contact or movement–not pain.
There is sometimes a belief that people who engage in sensory seeking activities like headbanging, slamming into objects or biting themselves are doing it because pain is the desired outcome and I don’t think that’s always true. It may be true for some, but for others, those activities don’t hurt, either due to pain hyposensitivity or an ability to regulate the level of contact in a way that keeps it below our pain threshold.
64 Flavors of Sensory Seeking
While I’m primarily a proprioceptive and vestibular sensory seeker, there other types of sensory input that I’m strongly drawn to:
touching surfaces and objects
the feeling of sound resonating in my chest (Tibetan singing bowl, trains, explosions in IMAX movies, loud music)
the exhaustion after a hard workout
the smell of fire
being immersed/floating in water
Of course, that’s me. Everyone’s sensory seeking preferences are different. Some common examples by category:
Tactile: seeking touch from others; touching objects, textures or surfaces (either certain types or everything)
Visual: seeking visual patterns, moving objects, specific colors or shapes
Oral: seeking food or nonfood objects to taste, chew or suck on; seeking specific sensations like crunchy, spicy, or minty
Olfactory: seeking specific preferred smells; smelling everything
Vestibular: spinning, rocking, being upside down; seeking specific head or body positions; jumping from heights; seeking intense speed or movement
Auditory: seeking loud, repetitive or specific types of noises; making sounds because they’re pleasing
Interoceptive: seeking bodily sensations like hunger, thirst, urgency to use the bathroom, fatigue
Proprioceptive: physical contact, crashing into things, stretching, pressure, sound resonance
But Why?
What drives to seek out our preferred sensory inputs? I haven’t been able to find much scientific background, so I have only my personal experiences to share:
Regulatory: As a kid, I think my intense sensory seeking behavior was a way of soothing my overloaded brain. There were many many days when I couldn’t wait to get home from school and ride my bike to the top of the highest hill in the neighborhood. The hard climb up and brain rattling ride down were the only way I knew to soothe the angry anxious restless feelings that built up during the day.
As an adult, I’m better at regulating myself in more typical ways. Still, after a long day in the city I like to wedge my body into a seat on the train so my legs are pressed up tight against the seat in front of me. I do the same thing on airplanes and long car rides. The pressure calms me and helps downregulate my sensory overload.
I’ve read that stimming and sensory seeking behavior can be stimulating (hence the term stimming) but I’m rarely in need of any added sensory stimulation. I usually have more than I can handle.
Connection: Sensory input reminds me that I have a corporeal form. It connects my mind to my body and my body to my environment in tangible ways. Without touch, pressure and movement, I can easily get disconnected from my physical self.
Organization: Some types of sensory input help me feel more organized and integrated. At the end of the day, when I’m watching TV, putting my weighted blanket over my legs keeps me from turning into a squirmy mess on the couch. Without the added weight on my legs, I’ll change positions every five minutes trying to get comfortable because my body feels so disorganized and physically confused by the end of the day.
Physical dissociation and disorganization are things I’ve only recently realized that I experience. I was going to write about them to help clarify the “why’s” of my sensory seeking but I wrote so much that it will have to be a separate post.
Not Growing Out of This One Either
I’ve always had strong sensory-seeking tendencies. I think I always will. This isn’t a bad thing. It’s actually one of the things I like about being autistic. I have the ability to experience certain sensations in ways that most people don’t.
I like the intensity and immediacy. I like the pleasure I can find in mundane everyday things like the rumble of a passing train or the feel of a matte bookcover. It’s not exactly a superpower, but does give the world around me a vivid tangible realness that I can tap into whenever I need to reconnect myself with my self.
Polly Flinders was the bane of my childhood. I hated her with a passion. Why? Because she made dresses like this that were all the rage for little girls in the seventies:
A classic Polly Flinders dress. I had one just like this, same color and all.
For a four-year-old with tactile defensiveness, that dress was an instrument of torture. I can still feel the exposed elastic biting into my upper arm, the scratchy lace prickling my skin, the rasp of the tag on the back of my neck, the smocking bunching up across my chest.
Thanks to Polly Flinders and her ilk, I was branded a tomboy early in life. Not because I didn’t like dresses, per se. The way clothing feels is ten times more important to me than how it looks and “boyish” clothes (jeans, plain cotton shirts) were more comfortable.
I still shop for clothing based on feel first and look second. Where a lot of women see exciting new outfits, I see this:
Thanks to my tactile sensitivities, I’m a defensive shopper when it comes to clothing.
Clothes shopping is a matter of eliminating the things I know will be too uncomfortable then choosing what I like from the remaining options. If there are any.
When I do find something I like–and by like, I mean something that’s comfortable–I tend to buy it in multiples. I have a rainbow of v-neck t-shirts and long sleeve tees, all exactly the same brand, style, material and cut. Last weekend, I found a soft comfy sweater at Old Navy and bought it in three different colors.
When I like something, I’ll wear it until it literally falls apart. The few things I really love–my favorite pair of jeans, my softest t-shirt–I put on as soon as they come out of the wash. They rarely get hung up in the closet.
That isn’t to say that I live in tees and jeans. I have some dressier clothes that are comfortable. I try to dress both comfortably and appropriately for the situation. You’re just not going to find me greeting my husband at the door in pearls and heels like June Cleaver. Continue reading Tactile Defensiveness→
Like a lot of what I experience because of Asperger’s, until I started reading about insomnia, I didn’t realize that I’ve suffered from it on and off since I was a child.
Apparently, I’ve always had slightly abnormal sleeping habits. Sometimes it takes me a long time to fall asleep. Some nights I wake up a half dozen times; others (like today) I wake up at 3:00 AM feeling like it’s the middle of the afternoon. I can hit the ground running at 5:00 AM with an energy level that seems to piss people off.
In more technical terms, I have classic signs of autism-related insomnia:
prolonged sleep latency (time to fall asleep)
reduced sleep efficiency (decreased time asleep/time in bed)
reduced total sleep time
reduced sleep duration and continuity
night awakening exemplified by of long periods of time awake1
I was shocked to learn that the prevalence of insomnia in children with ASD is 40% to 80%.2 When you read about typical symptoms of autism and Asperger’s, sleep disturbance is not only missing from the core list of diagnostic symptoms, it’s rarely mentioned at all.
What my clock read this morning when I woke up.
A Budding Insomniac
My parents adopted a benign disinterest when it came to my sleep habits. They put me in bed at eight o’clock and the rest was up to me. I’d make multiple trips to the bathroom for a drink of water or to take one last pee (three or four or more times) but as long I didn’t bother my parents, they didn’t make a fuss about whether I was actually sleeping.
I had a nightlight beside my bed and most nights I’d hang over the side of the bed, reading until I felt tired. Before I was old enough to read, I would sit at the top of the steps and listen to what was going on downstairs to pass the time until I felt tired. In my teens I got a portable black and white TV for my birthday and I’d watch TV, using earphones so I wouldn’t get caught.
I think my parents knew about these habits–they occasionally pointed out that I’d go blind if I kept up my “reading in the dark” and more than once they shooed me back to bed from the bottom of the steps. On an average night, though, my parents’ bedside lights had been turned off by the time I made my last couple of trips to the bathroom.
When I woke in the night, which happened most nights, I’d call my dad and he would lie down in my bed while I went to the bathroom. I’m not sure what purpose this served except that I remember being a little afraid of the dark after walking into a wall and getting a bloody nose one night. I guess it was reassuring to know that if I did it again, at least my dad would be there to hand me some tissues.
My parents’ laissez-faire attitude toward my sleep problems taught me two things: (1) it’s not a big deal and (2) you’re responsible for putting yourself to sleep. The second part sounds a bit harsh, but because they never made an issue out of when or how much I was actually sleeping, it never felt that way. A little lonely perhaps, but I also liked those few hours at night when everyone else was asleep and the house was quiet. I got to indulge in my special interest (reading) and that was calming, which eventually lulled me to sleep.
Granted, if I’d been destructive or intent on going out to roam the neighborhood, this strategy wouldn’t have worked.
What Works for Me
As an adult I’ve learned that having the right sleep conditions makes a big difference for me. Some things that help me sleep better:
1. Plenty of exercise during the day. I need to be physically tired to sleep well so getting in at least an hour of walking, running and/or swimming every day is essential.
2. Heavy blankets. The slight pressure of a heavy comforter and blankets relaxes me. If I only have a sheet or light blanket, I’ll wake up repeatedly.
3. A cool room. I tend to overheat when I sleep. I’m not sure if this is Aspergers-related, but if the room is even slightly warm, I’ll wake up sweating.
4. Comfortable clothes. As a kid I wore snug fitting pajamas. I still can’t sleep in anything that’s too loose, like a nightgown, because I end up feeling like it’s strangling me the first time I turn over.
5. Familiar surroundings. It’s much easier to relax when I’m in a familiar environment. If I go on vacation or move to a new place, it takes me a few days to “learn” to sleep there because my brain needs to catalog the unfamiliar sounds and smells.
6. A quiet environment or consistent noise. I need either total quiet or a consistent natural noise (wind, waves, steady traffic) to fall asleep. Something like intermittent voices, a radio or a television–even one playing in the apartment above or below me or in an adjoining hotel room–will keep me awake until it stops. In fact, I’ll usually be awake long after it stops because of the anxiety it generates.
7. A dark room. I can’t sleep unless the room is completely dark. Light shining in my room through a window or under/around a door will keep me up. The flashing light of a muted television drives me nuts.
8. Reading (or enjoying a special interest) before bed. Reading has been one of my special interests since childhood. Like any special interest, it distracts and calms me. I think it’s also become a sleep cue. When I pick up a book in bed, my brain starts sending out sleep signals to my body. It usually only takes 15-20 minutes of reading before I start to feel myself drifting off.
9. A light dinner and no snacks after dinner. I fall asleep faster and sleep better if I have a low-fat, low-sugar dinner and give myself at least a few hours to digest it before going to bed
Those are the things that I’ve discovered over the years work for me. I’d love to hear from others on the spectrum who’ve discovered tricks for getting to sleep or staying asleep.
Recently I was talking with my daughter about my sleep habits and she asked why I don’t try to resolve my insomnia. I told her that it doesn’t bother me–I use my middle-of-the-night time to read or think–or impact my daily life. Her response was, “Maybe it does impact you and you don’t realize it because you’re so used to it.” There’s a lot of wisdom in that statement. Something to think about, for sure.
(Unless you’re a geek like me, you can safely stop reading here.)
A Little Geekery About Melatonin and Circadian Rhythm to Wrap this Up
There are a few theories about why so many people with ASD have sleep problems. One of the most prevalent theories points to abnormal melatonin levels.2 Consequently, many children with ASD-related insomnia are given melatonin to induce more regular sleep habits. From what I’ve read anecdotally, this works well for many children and results in unacceptable side effects for some.
Another, lesser-known theory that caught my attention suggests that neurodevelopmental disorders increase the likelihood of sleep disturbances due to an inability to perceive and interpret sleep-related environmental cues.3 This is obviously far more difficult to measure and quantify in a lab than melatonin levels (which are easily measured in blood plasma). But it got me digging for more details because so much of my Asperger’s seems to trace back to the dysfunctional processing and filtering of my environment.
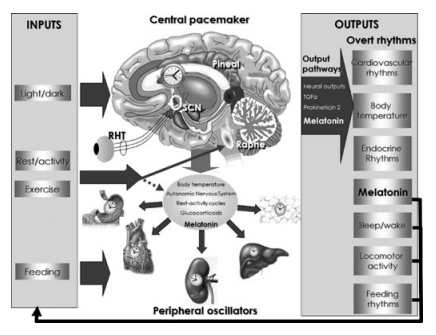
Caution: amateur scientist at play: I learned that our circadian rhythm (the internal clock responsible for, among other things, when we sleep) relies on external inputs to regulate sleep. The natural light-darkness cycle is the primary input, but our circadian rhythm can also be affected by our rest/activity schedule, mealtimes and social interaction. All of these inputs pass through a “central pacemaker” in the brain, which “outputs” various hormones that act as signals to the rest of the body and regulate the sleep-wake cycle.
Here’s a nifty graphic showing the “input” and “outputs” of the human circadian system4:
From “Exercise and melatonin in humans: reciprocal benefits” in Journal of Pineal Research by Escames et al.
The really interesting part is that the body can’t maintain an accurate 24-hour circadian rhythm without the input of environmental cues. Our natural circadian rhythm, in the absence of environmental cues, is 25-27 hours. Whoa!
Perhaps dysfunctional processing of one or more circadian inputs throws off the circadian rhythm, leading to the abnormal levels of melatonin (a key output) found in many people with ASD.
The dysfunctional processing theory would explain why many of the things I do to help me sleep better qualify as circadian inputs: exercise, consistent activity cues around bedtime, no eating close to bedtime, and a dark room. Over the years I’ve developed inputs that tell my body loud and clear: calm down and go to sleep.
It doesn’t always work but I have a feeling things could be a lot worse.
References:
1Goldman, Suzanne et al. “Parental Sleep Concerns in Autism Spectrum Disorders: Variations from Childhood to Adolescence” J. Autism Dev Disord, 2012, (42) 531-538.
2Souders MC; Mason TBA; Valladares O; Bucan M; Levy SE; Mandell DS; Weaver TE; Pinto-Martin D. Sleep behaviors and sleep quality in children with autism spectrum disorders. SLEEP 2009;32(12):1566-1578.
3Williams, P. Gail et al. “Sleep problems in children with autism” J. Sleep Res. (2004) 13, 265–268.
4Escames, G., Ozturk, G., Baño-Otálora, B., Pozo, M. J., Madrid, J. A., Reiter, R. J., Serrano, E., Concepción, M. and Acuña-Castroviejo, D. (2012), Exercise and melatonin in humans: reciprocal benefits. Journal of Pineal Research, 52: 1–11. doi: 10.1111/j.1600-079X.2011.00924.x