Dog training instructor: “Get excited! Look happier! Make your voice happy! You have to sound HAPPEEEEE! If you don’t sound HAAPPPPEEEEE!!! your dog won’t know that she’s doing it right.”
Random stranger, after a 5-minute phone conversation: “You don’t seem like a very nice person.”
The Scientist, after sharing something meaningful: “Do you have any feelings about what I just said?”
Phone interviewer, mid-conversation: “I’m glad I’m recording this. You talk so fast, I could never take reliable notes.”
Many people, in many situations: “Shhh. Keep your voice down. The whole floor/house/airport/neighborhood doesn’t need to hear your story.”
More people than I can count (sarcastically): “Don’t sound too excited about it.”
Who Needs Prosody? Not Me
The first time I ever heard the word prosody was when Jess was in high school. She went to a performing arts magnet school, where she majored in creative writing. Occasionally her report cards would mention that she was working on prosody as part of a poetry class.
This week’s test is more of an inventory of traits than a quantitative test. The SPD checklist is intended to help identify areas of atypical sensory processing, including hyposensitivity, hypersensitivity and sensory seeking.
Sensory processing disorder (SPD) is a stand alone diagnosis, however, there is substantial overlap between SPD and the atypical sensory processing that autistic people experience. In fact, now that sensory sensitivities are included in the DSM-5 diagnostic criteria for autism, we may start to see fewer kids getting diagnosed with SPD plus an alphabet soup of other conditions. Because the odds are really high that a kid with concurrent diagnoses of SPD, ADHD, and ODD is really just an autistic kid in disguise. But that’s a rant for another day. . .
I’ve written quite a bit about atypical sensory processing, so I’m going to get right to taking this week’s test.
Taking the Test
There several online versions of the SPD Checklist. The one I’m linking to for this post has a couple of nice features: it’s (mostly) worded as an adult checklist, it’s printable so you can complete it on paper, and the links at the top of the page allow you to filter the questions by type, in the event that you want to focus on just one area of sensory processing.
To get started, go to the SPD Checklist webpage. This a “paper and pencil test”, so your options are: print it out and sharpen your pencil, create a tally sheet to add up your scores, or copy/paste into a word processing application.
Edited to add: Anna very kindly made us a spreadsheet that totals up the scores for each section: SPD Checklist (recommend that you save it to your computer or make a copy before using it)
To take the test, read each item and numerically score it as follows:
0 – Never (not at all)
1 – Rarely (a little)
2 – Sometimes (moderately)
3 – Often (quite a lot)
4 – Always (severe)
I assigned words to the scale to help me better understand how to use the numerical scores. The instructions also say that you can score an item as P for “previously experienced but no longer present” however there is no explanation of to interpret P numerically.
Interpreting the Results
The checklist has 138 total items, for a total possible score ranging from 0 to 552. There are no guidelines available for interpreting the numeric scores and I think that’s because this checklist is meant to be a qualitative guide to a person’s sensory processing rather than an indication of a diagnostic threshold. Of course, I still couldn’t resist adding up my numerical scores.
The items on the checklist are divided into 8 categories:
General Modulation (scoring range: 0 – 36): The 9 items in this category are broad and were some of the hardest to answer because they felt so vague. I scored 22.
Over-Responsiveness (0 – 100): The 25 items here cover hypersensitivity to sensory stimulus, with a heavy emphasis on tactile and auditory sensitivities. I scored a 61, with the highest scores on tactile and general environmental items and the lowest on vestibular and taste items. No surprise there–I’m tactile defensive, easily overloaded by stimulating environments and a vestibular/proprioceptive/taste sensory seeker.
Under-Responsiveness (0 – 36): These 9 items cover hyposensitivity, mostly in the interoceptive category. I scored 13, with high scores on the interoceptive items and low scores on the rest.
Sensory Seeking (0 – 80): The 20 items in this category measure tendencies to intentionally seek out strong sensory experiences. I scored 48 + 1 P (knuckle cracking, which I did habitually as a teenager and have stopped doing). Most of my high scoring items are in the proprioceptive, vestibular and taste categories.
Sensory Discrimination (0-104): These 26 items relate to our ability to filter sensory information. I scored 42. This feels like the weakest area of the checklist. I know from experience that I have significant difficulty filtering sensory information but the items in this section didn’t accurately capture the difficulties I have. Difficulty licking an ice cream cone neatly? Not something I encounter on a daily basis.
Sensory Based Motor Abilities (0 -80): The 20 items in this category are related to fine and gross motor skills and would probably be more accurately described as such. I scored 41. Most of my high scores were in the area of fine motor skills.
Social and Emotional (0 – 88): I would classify this entire category as secondary traits because I think they’re more a product of having sensory sensitivities than “symptoms” of SPD. Also, this is where the line between autism and SPD becomes really fuzzy. There isn’t a single item among the 22 here that isn’t also an autistic trait or is strongly present in many autistic people. I scored 48, mostly due to high scores on the social and resistance to change items.
Internal Regulation (0 -28): This is another weak section. Difficulties with interoception are common in people with atypical sensory processing and the 7 items here were clearly written by someone who doesn’t experience interoceptive weirdness. I scored 17, with moderate scores on everything, simply because the questions are worded so vaguely. More questions with more specific traits would create a better picture of a respondent’s interoceptive issues. For example, “do you not realize that you need to use the bathroom if you are engaged in an interesting activity” or “do you sometimes forget to eat until you are feeling weak, dizzy or nauseous from hunger” would be much easier to answer than the current “under sensitive or over sensitive” wording.
Overall score (0 – 552): For what it’s worth, I scored 292 out of a possible 552. The overall score seems useless because, like an IQ score, it’s an aggregate of a set of disparate subscores.
The best approach is probably to look at the categories we score especially high or low on, and then drill down into the subsets of high/low scores within each category. For example, within the over responsiveness, under responsiveness and sensory seeking categories, there were clear patterns in my answers that identify which areas I’m hypo- and hypersensitive in.
This test also suffers at times from imprecise wording, making some of the questions hard to answer. I had no idea how to score “hates to be barefoot or hates to wear shoes/socks” because I prefer being barefoot and generally dislike shoes and socks, expect in situations where being barefoot would be painful. So is that 4 for disliking shoes and socks or a 0 for loving to be barefoot or what? Seems like a completely useless question. Same for “love to touch and be touched, have to touch everything.” Anyone who is simultaneously tactile seeking and tactile defensive knows that those are three completely different things.
The Bottom Line
The SPD checklist would benefit from the input of people who experience sensory sensitivities. A few of the questions felt unanswerable and some of the others could use refinement. However, completing the checklist can help someone with atypical sensory processing identify which areas they have the most challenges in. For those new to the concept of atypical sensory processing, it can also be a good introduction to the potential ways that atypical sensory processing affects our daily lives.
——-
Note: Take a Test Tuesday will be on hiatus for a while after today. I’m moving and not sure how long it will take for me to get settled in. Also, I’ve run out of test ideas again. If anyone has ideas for other tests that might be, let me know in the comments and I’ll start rebuilding a queue.
Before I get started, I want to thank ndsenseandsex for mentioning The Synesthesia Battery on Tumblr and inspiring this week’s Take a Test Tuesday post.
Even more importantly, I need to preface this by saying that I don’t have synesthesia. The background information for this test is based strictly on research and will probably be quite short. I know there are regular readers who are synesthetes. Perhaps they’ll provide us with some firsthand accounts of their experiences. Finally, if I’ve gotten anything here wrong, please tell me and I’ll edit as needed.
Okay, on with the test . . .
Synesthesia is a condition where one sense is automatically and involuntarily triggered by input to a different sensory channel. For example, watching a video of moving dots triggers an auditory sensory response or smelling a particular scent evokes a visual response, such a as a specific color.
There are a couple of key characteristics of synesthesia that differentiate it from simple sensory associations. Synesthesia “concurrents”–the atypical sensory responses that accompanies the typical sensory responses–are:
involuntary
consistent
automatic
This means that a certain type of sensory input always triggers the exact same concurrent response, whether you are consciously expecting it or not, and that’s been the case for as long as you’ve been a synesthete (usually since birth, except occasionally in the case of head injuries or drug-induced neurological changes).
There are many different types of synesthesia. Some people experience only one type of synesthesia and others experience multiple types. Some of the more common forms include:
numbers or letters are associated with colors
people (or the scents of individuals) are associated with colors
visual movement patterns are associated with sounds
sounds are associated with colors or other visuals
visual sights (other than food) are associated with tastes
pain is associated with colors
Synesthesia isn’t an autism trait, but anecdotally, there seems to be a high rate of synesthetes among people on the spectrum. Like autism, it also tends to run in families.
Taking the Synesthesia Battery
The test website has two components: a short pretest you can take to screen for synesthesia and a longer battery that tests for various forms of synesthesia. To take the test, start here. The 7-question screening pretest is optional. If you have no idea whether you might have synesthesia, it’s a quick way to get a better idea.
If you experience synesthesia and want to take the more comprehensive Synesthesia Battery, you’ll be asked to register by giving an email address. The site says that results will be anonymously added to a research database and that emails are kept private and never shared.
If you don’t want to register and take the Battery but are curious about what it consists of, there is a demo page with some screen shots and demo versions of the various parts of the test.
After registering and consenting to be part of the study, you’re asked to provide some demographic information. On the same page, you’ll be presented with a list of various types of synesthesia, with short descriptions of each, and asked to indicate which ones you experience. Based on which types of synesthesia you report experiencing, you’ll be served up a series of short tests.
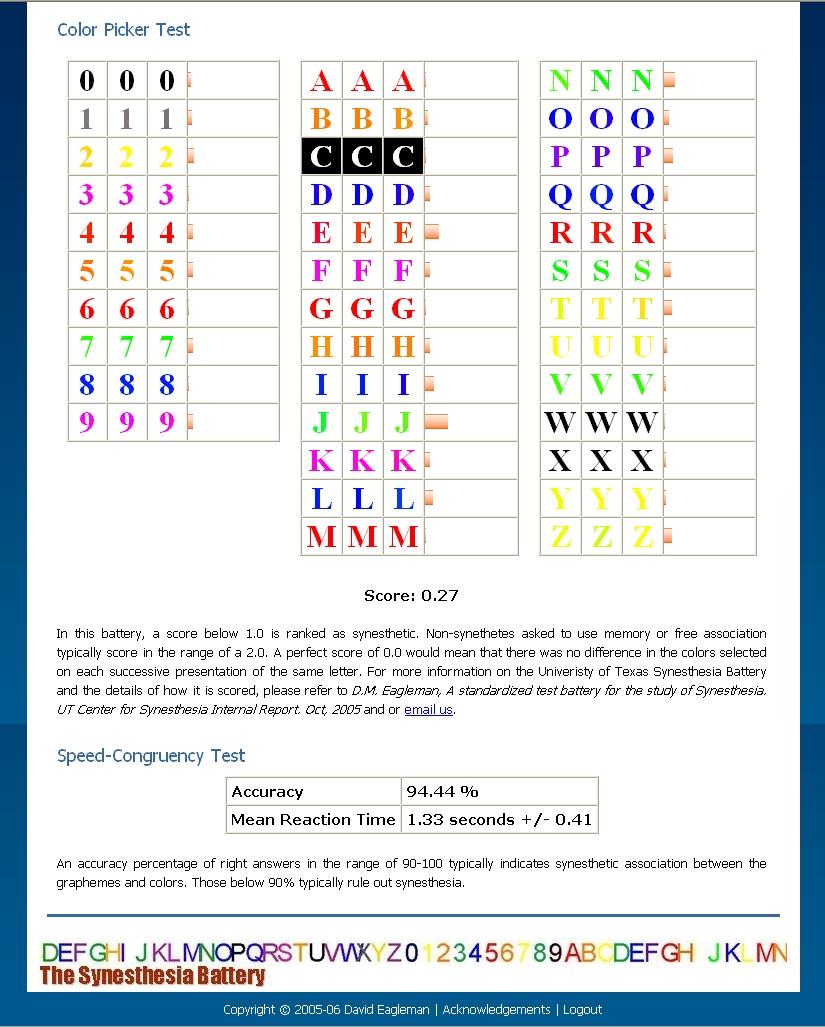
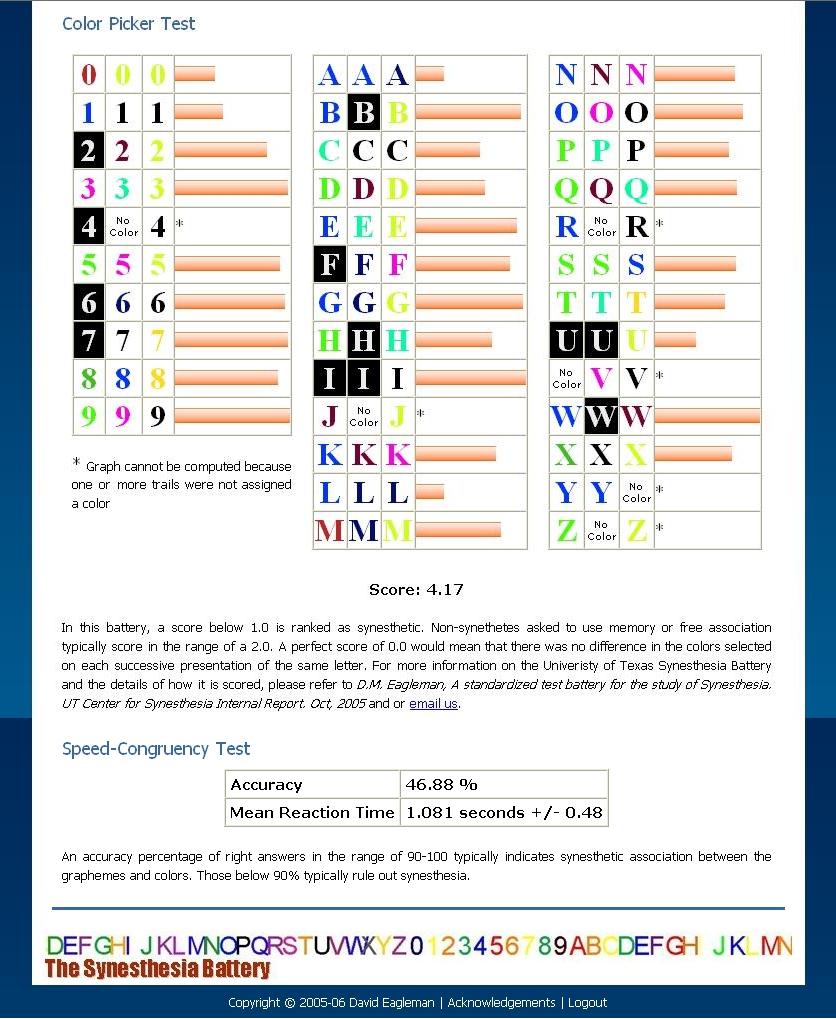
There are both interactive and question/answer tests. Each of the interactive tests lasts about 10 minutes. The interactive tests present a number of trials in which you’re asked to identify the concurrent for an item that is presented. For example, what color does M evoke or what color is this musical note associated with. The same “input” is repeated multiple times, testing how consistent your concurrents are.
The length of your test will depend on the number of tests that you’re given. You can stop at any time and come back to finish later by using the account you created when registering.
The Results
I didn’t take any complete any tests because I don’t experience synesthesia and didn’t want to contribute useless data to the study. I’m looking forward to hearing about any results that you all want to share with us.
There are quite a few synesthesia questionnaires available online, but the interactivity of this test adds a measure of objectivity that is hard to achieve with multiple choice questions alone. Obviously it’s impossible to test for certain kinds of synesthesia online, since our computers can’t produce scents or replicate all of the possible forms of sensory input that trigger certain kinds of synesthesia, but this test is similar to the ones used to test for synesthesia in clinical settings.
This is the final part in a series about sensory sensitivities and atypical sensory processing. Read the other parts: Part 1 | Part 2 | Part 3
When we think of diet or dieting, we usually think of restricting our intake in some way. But a sensory diet isn’t about restriction, it’s about fulfilling sensory needs and improving self-regulation with a specific selection of sensory activities.
The term sensory diet originated in the occupational therapy field and is commonly used in relation to both autism and sensory processing disorder. To create a sensory diet, an occupational therapist looks at a person’s areas of sensory hypo- and hyper-reactivity and comes up with ways to help up-regulate or down-regulate them.
This video has some great examples of the types of sensory activities that are often prescribed:
Going Up?
Sensory diet activities come in two flavors: upregulating and downregulating. Upregulating activities help to stimulate under-reactive senses. Downregulating activities, in contrast, help calm over-reactive senses.
Sometimes an activity that is upregulating for one person or in one situation can be downregulating for another person or in a different situation. For example, bouncing on a trampoline can stimulate the proprioceptive sensory channel but it can also help calm someone who is overloaded (by releasing excess energy). Continue reading Sensory Diet→
This is part 3 in a series about sensory sensitivities and atypical sensory processing. Read the other parts: Part 1 | Part 2 | Part 4
——-
While atypical sensory filtering is related to sensory sensitivities, not all unfiltered sensory data will trigger sensitivities. Remember the sounds I described hearing as I’m typing this? I’m not especially sensitive to any of them. I hear them and it’s hard to tune them out, but I don’t have a biological stress reaction to them. They’re just there and over the years I’ve grown used to having a lot of irrelevant aural data constantly pinging around in my brain.
In fact, I didn’t know until a couple of years ago that other people don’t hear all of those distinct ambient sounds when they’re engaged in an activity.
I suppose what’s happening in this case is my sensory gating is failing, letting the irrelevant sounds in. They get routed to an area of my brain that says, “oh, right, traffic, dog, sirens, rain, typing, closer traffic, harder rain, actually two dogs, footsteps upstairs” and on and on.
What should happen when I hear those repetitive background noises is something called habituation. The first time the dog down the hall barks, my filtering system might kick it upstairs to my decision making brain and say, “hey boss, is this something we need to worry about?” The decision making region would analyze the situation, decide that the dog is neither a threat nor any of my business, and say, “nope, ignore that from now on.” The filtering system would then flag that gate for closing, eventually tuning out the repetitive barking until I stopped noticing it.
This is part 2 in a series about sensory sensitivities and atypical sensory processing. Read the other parts: Part 1 | Part 3 | Part 4
——
I don’t like pistachios.
I have a sensory sensitivity to bright lights in a dark room.
What’s the difference between the two? I can eat pistachios if I have to. I won’t enjoy it, but if I happened to be served something that had some pistachios on or in it, I could eat it without having a negative biological reaction.
On the other hand, I can’t watch TV or look at a computer monitor in a dark room. The brightness of the screen is painful and my instinctive reaction is to look away or close my eyes. If The Scientist and I are watching TV at night, I need a small amount of ambient light to reduce the contrast between the television screen and the darkened room. Without it, I’ll squint at the screen and quickly develop a headache.
I know this because, like the t-shirt incident, I’ve tried to acclimate myself to watching TV in the dark.
I can see how someone who doesn’t know that I have sensory sensitivities might assume that I dislike watching TV in the dark in the same way that I dislike pistachios. If you’ve never experienced sensory sensitivities, it can be hard to believe that they’re real and that they have a biological component to them. But my body’s reaction to those two scenarios is very different. Continue reading The Difference Between a Sensory Sensitivity and Disliking Something→
This is the first in a series of posts about autistic sensory processing and sensory sensitivities. Part 2 | Part 3 | Part 4
—–
I once had a t-shirt that I really wanted to like. It was a souvenir from a trip to Hawaii. The color, the material, the fit, the design–all perfect. It would have been my favorite new shirt, except for one thing.
It had a tiny thread in the collar that scratched my neck. A thread so small that I couldn’t see it. I’d cut out the offending tag and all of the visible stitching holding the tag in place, but that one little thread refused to go.
So I decided that I was going to get used to it. I was going to pretend that evil remnant of plastic thread didn’t exist. If it was too small to see, surely I could ignore it.
I tried. I really did.
I put the shirt into my summer t-shirt rotation and wore it at least once a week. The material got softer with each washing, which only made me want to love it more. It was one of the most comfortable shirts I owned. It would have been that most elusive of things–the perfect shirt–except for that microscopic thread.
I developed seriously mixed feelings about the shirt. I was determined not to let the thread win. It became A Thing. Some days I would wear it all day, doggedly ignoring how the thread jabbed at the back of my neck when I moved this way or that way. Other days I’d only make it to early afternoon before tossing the shirt in the laundry and changing–with a sigh of relief–into a more comfortable shirt. One with the tag cut cleanly out.
This went on for years. I wore the shirt in spite of how it made my neck itch and burn, in spite of the way it made me unconsciously pull at my collar all day long. I wore it right up until the day I admitted to myself that I was never going to get used to that thread. Putting my Hawaii shirt in the donation bag felt like a defeat. A thread–so small it was invisible–had gotten the better of me. Continue reading Sensory Sensitivities and Atypical Sensory Processing→
I think I was born to be in motion. I have difficulty resting when I’m at rest.
If I have to sit in one place long enough, I’ll cycle through dozens of postures without thinking about it. I slouch. I splay. I pin one foot under the other. I pull one knee up, then two, hugging my shins with a hand or arm. I sit on my foot, ankle or calf. I sit crossed legged, even on chairs. I put my elbows on the table, lean my head or chin on my hand, interlace my hands on top of my head. I perch on the edge of my chair, turn sideways, tangle my feet in the legs of nearby furniture.
The variations are endless but they have one thing in common–they orient my body to my surroundings. Without a steady stream of proprioceptive feedback, I start to feel disoriented and disconnected from my body. I feel lost in space. Confused. Physically disorganized..
When I’m at home, sometimes I just go lie on the floor to give my body a break from being upright. Because being upright requires figuring out where to put my hands and arms and legs and feet and often no sooner do I get that all sorted out than that restless feeling starts nudging at my leg or foot or spine and I need to move again.
It’s not that I can’t sit like a proper adult. I often start out sitting with both feet on the ground, arms relaxed at my side. In fact, in new social situations, I make a conscious effort to sit properly. Because I’m not four years old. I’m an adult–often an adult in a situation where I’m expected to look professional–and adults have very specific expectations of other adults in those situations.
Often what I come up with is a tense variation of typical “good sitting posture”:
Then my internal clock starts ticking and one of two things happens. If I’m in a formal setting, my body will grow more and more tense as I work to maintain a polite, socially acceptable posture. Then I’ll start covertly stimming, rubbing something between my fingers or twisting my hand in my pantsleg, something to counterbalance the tension that’s building up as I force myself to be still.
If I’m in comfortable or casual surroundings, it doesn’t take more than five minutes for me to start shifting around, searching for a more comfortable position. On an airplane, for example, I’ll start out sitting with my feet on the floor, book in my hand, arms close to my sides–typical polite seatmate posture. Soon, I’ll have one leg splayed out along the aisle or tucked under my opposite thigh. When that stops working, I’ll slouch and pin both knees against the seat in front of me or turn sideways and pull my legs up to my chest or fold one leg across the knee of the other, wedging a foot against the seat in front of me.
The fact that I’ll start stimming when I can’t freely change my posture often probably indicates that the positions I use to feel comfortable are in fact themselves a form of stimming.
Reset, Relax, Repeat
My body has a time limit on any one position. Even when I’m trying to fall asleep, if I don’t nod off right away, I need to keep changing position every ten minutes or so.
When I’m still, I have a gradual build-up of . . . I don’t know what. Tension? Discomfort? Disorganization?
I start to feel more and more uncomfortable until I have an uncontrollable urge to rearrange myself. Once I move into a new position, I’ll feel comfortable–momentarily at rest. Then, gradually, the discomfort starts building and soon I have to move again. Sometimes it’s only a matter of shifting back and forth repeatedly between two positions–a trick I used a lot at university to avoid adopting too many odd slouchy postures in class.
As important as the movement–and here’s where I think the particularly autistic aspect of this comes into play–is the position of my limbs. I almost always have one part of my body pinned, pressed, squeezed or wedged against or under something–either another body part or a piece of furniture. I think this deliberate pressure creates feedback that grounds me physically. It reminds me of where my body is in space and makes me feel safe in a way I can’t describe with words.
Physically, pressure equals organization.
Perhaps it’s like swaddling a baby. Mothers have been snugly wrapping up fussy infants for centuries. There is some science to back up the practice, suggesting that swaddling calms babies by enhancing motor organization and self-regulation. Once babies reach a few months old, swaddling is no longer beneficial or necessary because they have a reduced startle reflex and better-developed motor control.
Maybe there’s something very primitively calming about the kind of pressure I’m constantly seeking–a sort of localized form of swaddling.
Or perhaps it’s simply about feedback. Given my poor sense of interoception and my strong drive for proprioceptive sensory input, it’s not surprising that I need to intentionally create a steady stream of input to remind me that I physically exist.
Let’s talk about interoception. I bet you’re already on the edge of your seat, right?
Okay, okay, first a definition. Interoception describes our sensitivity to sensations that originate in our bodies. Think pain, temperature, itch, sensual touch, sensations from our organs and muscles, hunger, thirst, and breathlessness.
All of these sensations combine to give us a sense of sentience. I’m hungry therefore I am.
Our Body’s Dashboard
Interoceptive feedback is important for keeping our bodies in good working condition. Think of them as the body’s dashboard. Are we low on fuel? Running too hot? Has it been too long since some critical service was performed or is a warning light flashing? Interoceptive sensations provide the feedback necessary for troubleshooting and correcting imbalances in the body.
Emotions often arise from our interoceptive sensations, too. When someone asks how you feel, you probably subconsciously check-in with your body, and realizing that you’re tired, hungry, hot, or achy, you reply, “not too great.” Or conversely, if your interoceptive sensations are in balance, you might report feeling happy or at least content.
Obviously not all emotions are tied to interoception, but it’s hard to be happy when you’re in pain or content when you’re itchy. For many people being hungry or tired is a direct route to being cranky and short-tempered. Those of us who are alexithymic experience this even more strongly, often struggling to identify the difference between emotions and physical sensations. I can’t explain how my body confuses “upset” with “cold,” but sometimes it does. Now I know that if I’m feeling cold when no one else around me is, I need to check in with my emotions. And put on a hoodie.
Engage Interoceptive Dampeners
But what if your interoceptive system is dampened? What if a sensation needs to be in the red zone before it comes up on the dashboard? Well, then you forget to eat or stare in wonder at your bleeding toes or don’t realize you might be in pain until you pass out. Sound familiar?
Many autistic people have dampened or muted interoception. We just don’t seem to notice what’s going on in our bodies until it reaches a level that other people would find intolerable. And often when we do notice it, it goes from “oh that’s happening” to intolerable really darn fast.
As often as I experience this in minor, inconvenient ways, I’m occasionally reminded of how dangerous it can be. Because hindsight is 20/20, I can see in retrospect that I recently had a UTI coming on for days before I picked up on the symptoms. One of the main symptoms is pain and other than a vague crampy feeling, I wasn’t experiencing any. Easy to ignore, so I did.
Then some harder to ignore symptoms started happening and my daughter, who I was visiting at the time, said, “you need to go get this checked now.” Left to my own devices, I probably would have taken a wait-and-see approach which would have been bad. Because a few hours later, shortly after getting my prescriptions filled, I was in intense pain. An hour early, at the walk-in clinic, the doctor asked me if I had any pain and, after thinking about it for a moment, I said, “maybe a little?”
My body had gone from zero to “MAKE IT STOP” in less than hour.
And thanks to my body’s poor interoceptive workings, I was rewarded with a kidney infection because unlike most women who dash off to the doctor at those first signs of a UTI, I wasn’t getting enough data to trigger my internal alarms. It wasn’t until I started having more obvious symptoms that I realized something might be wrong and took to Google to figure out what it could be. By the time I started getting the right antibiotics in my body, a common minor ailment has progressed to a potentially serious illness that I’m just starting to recover from two weeks later.
Unreliable Indicators
One of the purposes of interoception is to drive behavior.
Hungry? Eat.
Tired? Sleep.
Pain? Seek help.
Interoceptive sensations–especially pain–may be unreliable indicators in autistic individuals. Medical professionals often rely on pain and other self-reported symptoms of discomfort to assess the presence or seriousness of an illness. In my case, my interoceptive sensations were saying “meh” but my fever (which I didn’t realize I had) and high bacterial count were saying, “hey, big problem here!”
When you combine muted interoception with poor executive function–which may be further impaired by the stress of illness–you’ve got a recipe for disaster. This is why I need someone else to say, “we’re going to the doctor now.” It’s also why recognizing that autistic people may have unique pain, distress or illness signals is important for medical professionals, caregivers and loved ones. This can potentially lead to misdiagnosis or underdiagnosis.
Our nonstandard brain wiring can mean that we miss common warning signs or have difficulty knowing when to act on distress signals.
The summer before seventh grade I went to an amusement park with my cousins. Until that day, my amusement park experience had been limited to kiddie rides. My parents weren’t roller-coaster-riding types and I guess they assumed I wasn’t either.
So there I was, first time in a real amusement park with real rides and roller coasters and everything and I was . . . terrified. I felt sick to my stomach just looking at the rides. But my cousins, who had been to the park many times, grabbed my hands and made a beeline straight for a ride that looked like this:
It was called Strawberry Fields and as we waited for it to start, songs from “Sgt. Pepper’s Lonely Heart’s Club Band” blared from the speakers overhead. My memory of that moment is clear as if it happened yesterday. I can hear the scratchy version of “Lucy in the Sky with Diamonds”, feel the greasy vinyl of the safety bar beneath my sweaty palms and practically taste my fear as my heart galloped in my chest.
And then we started to move, slowly at first, gaining speed, a little more and a little more until the wind was whipping my hair across my face and the three of us were pressed in a bone-crunching heap against the outside of the car and I was screaming right along with everyone else through 90 seconds of pure, unadulterated joy.
When the ride stopped all I could think was, “holy shit, let’s do that again!” And again and again and again.
I’d discovered one of my favorite sensory experiences: going fast. Blindingly fast. Mind-numbingly fast. The speed was exhilarating. I rode everything in the park. The faster it went, the more I liked it. Spinning, falling, dipping, swinging–I had no idea why I liked the intense physical sensations that the rides created, but I did. When I went back to the park on a seventh grade field trip, I spent the morning riding a roller coaster, jumping off and running around to the entrance to get right back in line.
Sensory Seeking =/= Stimming?
Now that I know about sensory seeking behavior, my sudden intense love of amusement park rides makes sense. Autistic people are often sensory seeking in a big way. We have a strong need for intense sensory input and will deliberately seek out or create sensory experiences to satisfy that need.
Sensory seeking is often described as a way to either stimulate an understimulated nervous system or calm an overstimulated system. Which sounds a lot like the typical definition of autistic stimming.
That raises the question: is sensory seeking behavior a form of stimming? There is a lot of overlap between the two, but I don’t think they’re identical. Stimming provides sensory input so I think we can say that all stimming is sensory seeking. But stimming is generally repetitive, which isn’t always true of sensory seeking.
Going on a roller coaster once or twice? Probably sensory seeking. Going on a roller coaster twenty times in a row? Could be stimming.
Honestly, I have no idea. Feel free to weigh in with your own theory, opinion or confusion in the comments.
The Wild Ones
Much of my childhood play was sensory seeking in disguise. Some of my favorite activities as a kid:
Going as fast as I could down big hills on my bike, roller skates or sled
Jumping or diving off the high board
Hanging upside down and doing somersaults on the monkey bars
Jumping on the bed (broke my jaw doing this)
Bouncing on a trampoline or Hippity Hop
Sit ‘n spin!
Climbing trees and hanging upside down from the branches or jumping to the ground
Running into the padded gymnasium wall and bouncing off
Zipping my arms into my coat and playing crash dummies with a friend (this never ended welll)
Lying underneath my beanbag chair while watching TV
Swinging as high as I could on the swings then flying off
These are not especially “girly” pastimes. They’ll get you branded a tomboy and a handful. If you’re a boy, you’ll be seen as wild and unruly, maybe you’ll get an ADHD diagnosis.
My next door neighbor had a Hippity Hop and Sit ‘n Spin–neither of which my parents would buy me. I didn’t especially like my neighbor but I loved her toys.
As a teenager I took up martial arts, primarily for the self-defense aspect of it, but I discovered that I liked the contact that sparring involves. Getting hit while padded up with gear creates a very tangible kind of physical feedback. So does pounding a heavy bag or kicking a hand target hundreds of times in a row.
Although that may sound masochistic, it’s not. I don’t seek out pain. Let’s be clear about that. Although I often engage in activities that have a risk of injury and pain, what I’m looking for is a benign physical sensation–one of pressure or contact or movement–not pain.
There is sometimes a belief that people who engage in sensory seeking activities like headbanging, slamming into objects or biting themselves are doing it because pain is the desired outcome and I don’t think that’s always true. It may be true for some, but for others, those activities don’t hurt, either due to pain hyposensitivity or an ability to regulate the level of contact in a way that keeps it below our pain threshold.
64 Flavors of Sensory Seeking
While I’m primarily a proprioceptive and vestibular sensory seeker, there other types of sensory input that I’m strongly drawn to:
touching surfaces and objects
the feeling of sound resonating in my chest (Tibetan singing bowl, trains, explosions in IMAX movies, loud music)
the exhaustion after a hard workout
the smell of fire
being immersed/floating in water
Of course, that’s me. Everyone’s sensory seeking preferences are different. Some common examples by category:
Tactile: seeking touch from others; touching objects, textures or surfaces (either certain types or everything)
Visual: seeking visual patterns, moving objects, specific colors or shapes
Oral: seeking food or nonfood objects to taste, chew or suck on; seeking specific sensations like crunchy, spicy, or minty
Olfactory: seeking specific preferred smells; smelling everything
Vestibular: spinning, rocking, being upside down; seeking specific head or body positions; jumping from heights; seeking intense speed or movement
Auditory: seeking loud, repetitive or specific types of noises; making sounds because they’re pleasing
Interoceptive: seeking bodily sensations like hunger, thirst, urgency to use the bathroom, fatigue
Proprioceptive: physical contact, crashing into things, stretching, pressure, sound resonance
But Why?
What drives to seek out our preferred sensory inputs? I haven’t been able to find much scientific background, so I have only my personal experiences to share:
Regulatory: As a kid, I think my intense sensory seeking behavior was a way of soothing my overloaded brain. There were many many days when I couldn’t wait to get home from school and ride my bike to the top of the highest hill in the neighborhood. The hard climb up and brain rattling ride down were the only way I knew to soothe the angry anxious restless feelings that built up during the day.
As an adult, I’m better at regulating myself in more typical ways. Still, after a long day in the city I like to wedge my body into a seat on the train so my legs are pressed up tight against the seat in front of me. I do the same thing on airplanes and long car rides. The pressure calms me and helps downregulate my sensory overload.
I’ve read that stimming and sensory seeking behavior can be stimulating (hence the term stimming) but I’m rarely in need of any added sensory stimulation. I usually have more than I can handle.
Connection: Sensory input reminds me that I have a corporeal form. It connects my mind to my body and my body to my environment in tangible ways. Without touch, pressure and movement, I can easily get disconnected from my physical self.
Organization: Some types of sensory input help me feel more organized and integrated. At the end of the day, when I’m watching TV, putting my weighted blanket over my legs keeps me from turning into a squirmy mess on the couch. Without the added weight on my legs, I’ll change positions every five minutes trying to get comfortable because my body feels so disorganized and physically confused by the end of the day.
Physical dissociation and disorganization are things I’ve only recently realized that I experience. I was going to write about them to help clarify the “why’s” of my sensory seeking but I wrote so much that it will have to be a separate post.
Not Growing Out of This One Either
I’ve always had strong sensory-seeking tendencies. I think I always will. This isn’t a bad thing. It’s actually one of the things I like about being autistic. I have the ability to experience certain sensations in ways that most people don’t.
I like the intensity and immediacy. I like the pleasure I can find in mundane everyday things like the rumble of a passing train or the feel of a matte bookcover. It’s not exactly a superpower, but does give the world around me a vivid tangible realness that I can tap into whenever I need to reconnect myself with my self.












{kind=link}
{kind=link}