If you’ve read through the components of my ASD evaluation, you might be wondering but what about the Asperger’s questionnaire?
There wasn’t one. I didn’t complete a written screening or diagnostic test like the RAADS-R or AQ. My ASD diagnosis was based on the diagnostic interview, the outcomes of the cognitive/neuropsychological testing and behavioral observations made by Dr. H and B during my visit.
However, between the diagnostic interview and the behavioral observation, the key questions on the screening instruments were addressed in detail. The diagnostic interview covered questions on my special interests, relationships, social preferences, sensory sensitivities, attention, language pragmatics and fine motor skills. The behavioral observation included general presentation (grooming and dress), gait, speech (rhythm, rate and volume), demeanor, verbal skills, eye contact, movement patterns and conversation habits.
The interview and testing took about five and half hours. It was exhausting. We went straight through lunch, though both B and Dr. H told me that I could ask for a break at any time. The thing is, when I’m that engaged in something, I forget that I need to eat. I may be hungry, but the hunger signal gets muted.
So, exhausted and hungry, wishing I’d taken The Scientist up on his offer of a ride, I scheduled my follow-up appointment and stumbled out to the car. My evaluation was done. In three weeks I’d have a diagnosis.
Or not.
A vague sense of panic settled in as I started rehashing every detail of the appointment. Worse, I knew that I had three weeks ahead of me to perseverate on what I’d said and done and not said and not done. Three weeks to wonder if I’d done “too well” on the cognitive tests, if I’d instinctively made an effort to “pass” in the interview, if I’d withheld key details or reflexively covered my weaknesses.
Three whole weeks to alternately tell myself that this had been the best and the worst thing I’d ever done for myself.
The days passed about as quickly as you’d expect. I was restless and unsettled, plagued by a string of nightmares. The idea that Asperger’s might be something I’d talked myself into or imagined haunted me. My biggest fear–the one I couldn’t shake–was that Dr. H would tell me I wasn’t autistic, that in fact there was nothing wrong with me.
Then what? I’d found this explanation that fit so well. If someone “officially” took it away from me, I would be lost again, left to start over in search of a new, better explanation.
A few words of preface to this piece: I grew up as undiagnosed autistic with a gifted label, so my experience is different from what doubly exceptional children today experience. There were no social stories or social skills classes when I was a kid. Asperger’s Syndrome didn’t become an official diagnosis until I was 25. If you’re younger than I am and grew up with the doubly exceptional label or you have a child who is doubly exceptional, I’d love to hear about the differences or similarities in your/their experience.
—————-
Remember how, back when you were in school, there was one day of the week that was better than all the others? Maybe it was pizza day or the day you had band practice or art class. There was always one day that you looked forward to all week, right?
In sixth grade, for me that day was Friday. On Friday, I got to leave my regular classroom and walk down the hall to the TAG classroom. TAG stood for Talented and Gifted–a town-wide pilot program that accepted two sixth graders from each of the five elementary schools in our small suburb.
Ten geeks, eight of whom were boys. Ten kids who happily poured over reference books on Blitzkrieg and backgammon while the rest of the town’s sixth graders were wrestling with the math and reading curriculum we’d finished the year before.
Looking back, in addition to being gifted, most of us were probably on the spectrum as well. We were all socially awkward to some degree. None of us had to be asked twice to choose a topic for our Type III independent research projects. We came to class lugging backpacks filled with resources. We had entire libraries at home on the subjects we wanted to explore.
No matter what we asked to study, Mr. M, the aging hippie who taught the class, encouraged us. When I told him I wanted to “study” MAD magazine for my second project, he explained the concept of satire and helped me work out why the comics were funny.
Alfred E. Neuman and his famous tagline
TAG was aspie heaven. If I spent the afternoon curled up in a beanbag with my stack of MAD magazines, no told me to return to my seat. If I was the only kid in the class who brought a bag lunch because I couldn’t stomach the school pizza, no one at the lunch table made fun of me. If I needed to have a joke explained, even a whole magazine full of them, there was Mr. M, sitting at his desk, ready to patiently answer our questions with humor and honesty and not an ounce of condescension.
He thought we were the coolest kids around and in that classroom, we thought we were too.
Doubly Exceptional
Today, kids like the ones I shared the TAG classroom with are labeled doubly exceptional or twice exceptional. Back then we were the geeks and the nerds. Particularly if you were a girl and you were smart, people seemed to expect you to be weird. “Normal” girls weren’t smart and smart girls were quirky.
Adults wrote off our quirks as a byproduct of our intelligence. They sent us out to the playground and expected us to figure out how to navigate the social minefields that lurked within kickball games and jump rope circles. We were smart. We would get it eventually. When we didn’t, they reminded themselves that we were smart and because we were smart, we would get by.
And we did, but not always in the way they hoped we would.
As the concept of giftedness evolved, some theorists put forth the idea of giftedness as “asynchronous development,” suggesting that gifted children reach intellectual milestones faster than other children but lag in cognitive, social and emotional development. Proponents of this theory say that children who are hyperlexic, for example, develop in a fundamentally different way because they have access to advanced ideas at an earlier age than other children.
While this may be true of some gifted children, for many it serves to shift the focus away from their developmental disability–explaining it away as a byproduct of their giftedness. It’s easy to look at this model and assume that these children will just magically catch up with their peers developmentally. After all, they’re smarter than their peers. What’s keeping them from being just as adept in the social and emotional realms?
This is a bit like taking a kid who’s a good baseball player, throwing him in the pool, then being surprised if he sinks like a rock. What do you mean he can’t swim? If he’s athletic enough to hit a baseball, surely he’s athletic enough to swim.
Does my metaphor of a drowning child seem extreme?
If you spent your recesses and bus rides and summers at camp getting mercilessly bullied, physically threatened or worse, you probably wouldn’t think so. For kids who are developmentally disabled but intellectually gifted, expecting them to get by on intelligence alone is the equivalent of throwing them in the deep end of the pool without teaching them to swim first. It’s leaving them to drown–emotionally and mentally–all the while telling them how smart they are.
When a Strength Isn’t Always a Strength
Not that encouraging intellectual strengths is a bad thing. Unlike kids labeled developmentally disabled and given a deficit-based course of therapy designed to “fix” them, doubly exceptional kids have an advantage in their intelligence. It allows them to mask a huge portion of their disability.
Oh, wait–is that really an advantage?
Masking our disability with coping strategies and adaptations means that when we fail to hide something, people assume we’re not trying hard enough. Or we’re being deliberately obstinate. Or that we’re lazy, defiant, insolent, shy, ditzy, or scatterbrained.
“What’s wrong with you?” they ask incredulously. “You can memorize the batting averages of the entire Major League, but you can’t remember to put your homework in your backpack?”
And so the doubly exceptional child grows up thinking, “If only I tried a little harder . . .”
No matter how hard she tries, the refrain never changes.
Can’t hold down a job. Can’t finish a degree. Can’t maintain a relationship. Can’t seem to do the things an average adult can do.
“What’s wrong with you?”
If only I try a little harder . . .
Now What?
There is no gifted class in adulthood. No one cares if you can memorize all 20 spelling words after looking at them once. You don’t get to escape life on Fridays, reading MAD magazine while the sounds of the playground drift in through the open windows.
When you arrive in adulthood lacking the social skills that most people have mastered by sixth grade, life becomes exponentially more confusing and hard to navigate. For much of my adulthood, I’ve had the odd belief that someday I would “grow up” and suddenly feel like an adult. That I was just a little behind the curve when it came to social skills and one day everything would magically fall into place.
I don’t know when or how I was expecting this to happen. It’s illogical. Maybe it stems from the belief that social skills are intuitive rather than a skill set that needs to be learned.
Neurotypical people acquire social skills primarily by absorption; autistic people need to be taught social skills explicitly. When we’re not, we’re no more likely to learn them intuitively than a typical person is to pick up algebra intuitively.
Maybe that’s where the problem lies. Adults often assume that if a kid is smart enough to learn algebra in elementary school, he or she is smart enough to figure out social rules too. But who would expect the reverse to be true? What rational adult would say to their kid, “you’re smart enough to find friends to sit with at lunch, why can’t you figure out how to solve this linear equation yourself?”
I (Actually Don’t) Know What You’re Thinking
Even as I write this, I find myself cringing internally. Do I sound like a whiner? Shouldn’t I be thankful for the advantages my intelligence gives me?
Again, I find myself arriving at the notion that if I just tried harder, just applied the intellectual resources I have, I’d be fine.
Yes, intelligence helps. In particular, it helps me identify patterns and come up with rules–rules that any neurotypical adult could tell me, if I asked them.
If I thought to ask. Which I often don’t.
For example, at a get-together at a neighbor’s house, I accidentally knocked over a wine glass. The glass broke; I apologized.
Years later, while reading an etiquette book, I learned that I should have offered to replace the glass. This sounds like common sense now, but it’s not a rule I would have intuited or even thought to ask someone about.
Perhaps this is why the invitations for drinks at that neighbor’s home abruptly stopped? Did they find me insufferably rude? I have no idea.
Worse, when I mentioned the rule to my daughter, she frowned and said, “You didn’t know that?”
There are hundreds of unwritten social rules like this one. I have no idea how people learn them. Perhaps they don’t. Perhaps after a certain point, it becomes all about the dreaded perspective taking. You break a glass and think, “If I were the hostess, what would I want my guest to do to make this better?” And the obvious answer, when I think about it like that, is “offer to compensate for the loss.”
One Rule at a Time
Generally, I learn a social rule by reading about it, having someone explain it to me or seeing it in action. Unfortunately, many rules are executed privately, so there is no chance for me to observe them. The polite guest gets the hostess alone in the kitchen and asks about the cost of replacing the glass. (So says Emily Post.)
Even more frustrating: I’ve had people offer to replace something that was broken at my home. To me, that rule is, “If a guest breaks something in my home, they’ll offer to pay for it.” I don’t instinctively reverse the rule to apply to myself as the guest. If you’ve heard it said that autistic people aren’t good at generalizing, well, there you go.
There’s something at work here that has nothing to do with intelligence.
I’m smart and I’m developmentally disabled. One does not cancel out the other.
This week I took the Famous Faces, which tests for prosopagnosia or faceblindness.
Prosopagnosia, commonly known as faceblindness or facial agnosia, is an impairment in the ability to recognize faces. Although there isn’t a lot of research to support a conclusive link between ASD and prosopagnosia, some degree of faceblindness seems to be common in people with Asperger’s.
Some of the signs of prosopagnosia:
Failure to recognize a friend or family member, especially when you encounter them unexpectedly
Tendency to remember or recognize people based on their hairstyle, gait, voice or other defining non-facial feature
Relying features like hair style/color, facial hair or eyeglasses to recognize people you know well
Failure to recognize people out of context
Failure to recognize yourself in the mirror or in photos
I have all of these except the last one. If my daughter changes her hairstyle or I haven’t seen her in a while, I won’t recognize her right away. I locate my husband in a crowded place by the way he walks, what he’s wearing or his voice.
I rarely recognize people out of context and have actually said to more than one person, “Sorry, I didn’t recognize you out of context.” And that was before I knew anything about faceblindness.
For now, I’ll leave the background on faceblindness short because in researching this test, I found enough information for at least one more post.
Measuring Prosopagnosia
I’ve seen three different types of tests that “measure” prosopagnosia. One is a famous faces test which removes hair and other identifying features from the faces of famous people, requiring you to identity them by facial features alone.
Another type of test shows a series of faces and asks you to identify which of them belong to a set of 20 faces viewed at the start of the test. I took one online (sadly it’s no longer available) and came out in the bottom 20% of scores. My poor working memory probably didn’t help.
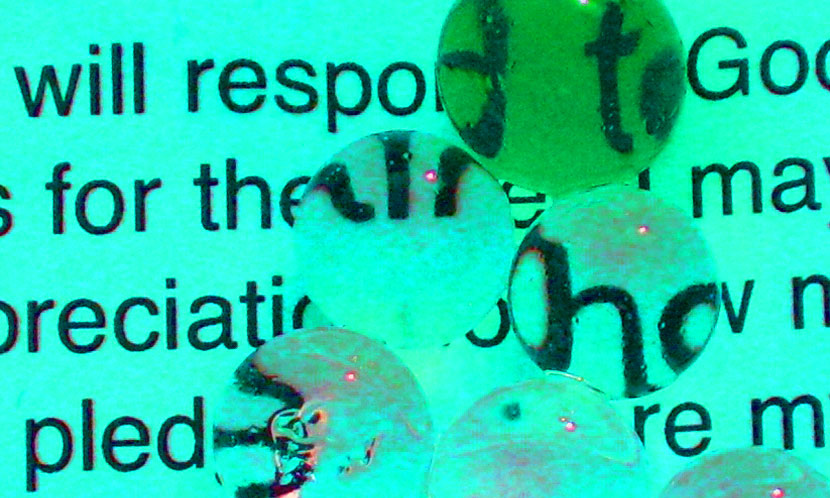
Finally, there is a type of test that digitally alters a face and asks you identify what is “wrong” with the face or which face among three (1 altered and 2 not) is different. This measures your ability to recognize “normal” vs. “abnormal” facial structure, a task that is easier for people who aren’t faceblind.
For example, can you tell at a glance what is wrong with two of the three faces below (answer in the caption):
The face on the left has closer-set eyes and the face on the right has a raised mouth. The middle face is unaltered. (Barton et al, 2004)
All of these tests obviously have flaws. A better test might be a series of questions based on the list of prosopagnosia traits, but that doesn’t seem to exist. There is a visual test that is supposed to be accurate at diagnosing prosopagnosia but it’s more time-consuming–we can take that one if folks are interested.
Taking the Test
You can take the Famous Faces test at Test My Brain. Choose it from the list of available tests, agree to the terms and answer the short demographic survey. There are 20 celebrities to identify–it took me about 10 minutes to finish but some of the faces I needed to study for a while, trying to picture them with varying hairstyles, before I could come up with a guess.
Scoring the Test
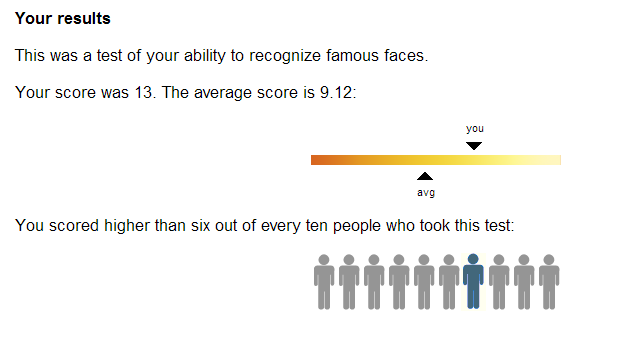
I did well, but my results may have been influenced by the fact that I’ve taken this test before.
I scored slightly above average but I had an advantage because I’ve taken the test before.
The first time I took Famous Faces, I thought George Clooney was Sean Connery and I mistook Nicole Kidman for Rosie O’Donnell. This time around I got George Clooney right but still missed Nicole Kidman. I also got Angelina Jolie, David Beckham, Fred Astaire, John F Kennedy Jr, Uma Thurman and Susan Sarandon wrong. If the photos had included hair I probably would have missed Uma Thurman, Nicole Kidman (because most blonde white actresses look alike to me) and David Beckham (unless his tattooed torso was included!).
The Bottom Line
The reliability of using famous faces tests to actually diagnose prosopagnosia is poor, but a low score may be indicative of some degree of faceblindness. If there’s enough interest, I’ll hunt down and do a write up on a more reliable test that’s used for clinical diagnosis of prosopagnosia.
This is Part 9 in the I Think I Might Be Autistic series. In Part 8 I covered the diagnostic interview portion of my autism evaluation and in this part I’m covering the cognitive tests, ADHD test and psychological screening questionnaires.
Cognitive Testing
Cognitive testing for ASD is a mix of verbal and nonverbal tests.
Some I found easy; others were a challenge. One actually made me bang my head on the desk, though I stopped as soon as I realized I was doing it because . . . inappropriate. Most were designed to start out easy and scale up in difficulty so that the last few were very challenging.
If you’re planning to be evaluated, you may or may not want to read about the tests I took in detail. Consider this your spoiler warning.
Here is a list of the tests I took with a short description of each:
WAIS-IV (full): An adult IQ test that measures verbal comprehension, perceptual reasoning, working memory and processing speed.
The verbal portion covered things like describing the similarities between two words (i.e. anchor and fence, statue and poem, allow and restrict), defining vocabulary words and answering general information questions. I found the “similarities” test challenging because some of the pairs had conceptual rather than concrete similarities. The other two sections were fairly easy because I’m both a walking dictionary and an encyclopedia of random facts.
The perceptual reasoning portion was a series of visual puzzles: using colored blocks to reproduce a design, deducing which design comes next in a series, and choosing shapes to form a larger shape. These tests were fun, although I found myself guessing at times.
The working memory tests involved repeating back strings of digits in forward and reverse order and doing math problems verbally. By the end of the digit string tests I was rocking back and forth in my chair with my eyes closed tight. The math problems, on the other hand, were fun. All of these tests made me conscious of how much I talk out loud to myself when my brain is working hard.
The processing speed portion involved locating symbols and coding a series of numbers into symbols. These were both fairly straight-forward pattern recognition tests that required balancing speed and accuracy.
Woodcock-Johnson III (partial): A test of academic skills that included orally identifying written words, orally spelling words given by oral prompt, and doing some math problems on paper, ranging from pre-algebra to basic calculus. I got tripped up by “questionnaire” on the spelling test. It’s one of those words that I always use autocorrect on. There is no autocorrect on an oral spelling test.
Wechsler Memory Scale IV (partial): The portion of this I took tested auditory memory. It involved two parts:
listening to a brief factual story and retelling it, including as many facts as possible, then responding with true/false answers to factual questions about the story (two trials)
listening to a long list of word pairs and then responding to a word prompt with the correct paired word (interminable number of trials)
I struggled mightily with both of these. My working memory is poor, especially when working verbally under pressure.
Rey-Osterrieth Complex Figure test: A measure of organization and planning skills as well as fine motor skills. It involves reproducing a complex drawing using a series of colored pencils that allow the evaluator to track the order in which the figure was drawn as well as the accuracy of reproduction.
Thirty minutes later, without any warning, I was asked to reproduce the same figure from memory. This did not go well. If you looked at the sample figure I linked to above, what I managed to reproduce the second time was basically a box with an X through it, a flag sticking out the front and bowling ball floating in the upper right corner. Bizarrely, I still remember exactly what it looked like and could draw that from memory months later.
Word Fluency: A timed test in which I had to think of as many words as possible that fit the following categories: animals, words starting with A, words starting with F, and words starting with S. These were challenging–I started out with a good head of steam but once I lost my momentum, I started perseverating on the words I’d already named instead of thinking of new words. Until I realized that I could name things from around the room that fit the prompt. Aspie adaptation for the win.
California Verbal Learning Test: Another test involving recalling items from a list with multiple trials. Again, I struggled with this one. The correct strategy, which I realized on the fourth trial, was to chunk the words by category to make recalling them easier. There were only five or six trials, so my realization came kind of late. This test also had me closing my eyes and talking to myself out loud because I was so frustrated with how difficult it was. There might have been some cursing. I was getting tired.
Trailmaking test: A connect the dots type of test–first connecting numbers only and then connecting an alternating sequence of numbers and letters. This measures visual scanning and sequencing ability. Surprisingly, I was quicker at the second series, even though it was the more difficult task.
verbally reading off a list of color words (blue, red, green) printed in black ink
verbally giving the color of a series of Xs there were printed in blue, red or green ink
verbally reading a list of color words, with each printed in a different color ink (i.e. RED printed in blue ink)
This test was deceptively easy. So much so, that when I saw my results, I was shocked. I scored in the “impaired” range on the first two and in the “high average” range on the third (and hardest) test.
Performing better on the more challenging versions of the Stroop and trailmaking tests leads me to believe that I’m more motivated to perform accurately on challenging tasks and if a task is too simple, I get bored and easily distracted.
Other Neuropsychological Tests
Grooved Pegboard test: A timed test of fine motor skills that consists of putting metal pegs in a pegboard, first with the right hand and then with the left. The only problem I had with this one was accidentally switching back to the right-handed order of inserting the pegs (right-to-left) when I was doing the left-handed test (meant to be completed left-to-right).
Reciprocal Motor Programs test: A test of how well I could repeat and then reverse repeat a series of finger taps.
ADHD Test
IVA Continuous Performance Test: This was the only cognitive test conducted by computer. The computer provided visual and auditory prompts at random intervals. If the prompt was a 1, I had to click the mouse. If the prompt was a 2, I had to refrain from clicking. The test was 21 minutes long. By the halfway point, I was stimming ferociously. I was also determined to ace this test (out of fear of being misdiagnosed with ADHD perhaps) so first I pretended that I was an air traffic controller and if I missed a cue, an airplane would crash. When that stopped working, I told myself that if I missed a cue, a puppy would die. Yeah, I take this stuff way too seriously. It took me awhile to wind down after this test was over because I sent myself into a state of extreme hyperfocus.
Questionnaires
I also completed four self-report questionnaires:
MCMI-III: This consisted of 180 true-false questions that test for 14 personality disorders (e.g. schizoid, depressive, compulsive) and 10 clinical syndromes (e.g. anxiety, bipolar, PTSD). There were also some funny questions, like “I am currently in an airplane” meant to verify that I was paying attention. Or not delusional. Hard to say.
Beck Depression Inventory (BDI-II): A 21-question self-report instrument for measuring the severity of depression.
Beck Anxiety Inventory (BAI): A 21-question self-report instrument for measuring the severity of anxiety.
Current and Childhood ADHD self-report: A self-report instrument for measuring the presence of ADHD symptoms now and during childhood.
I’ve mentioned my “missing word problem” here before. You may have noticed it in reading the blog or my comment replies–my tendency to skip over a small but necessary word when I write. This is more than a simple problem with typos, which I can easily catch and fix when proofreading.
The mystery of the missing words had proved intractable enough that I’d given up on solving it.
Until now, that is! I’m reading “The Mind’s Eye” by Oliver Sacks and right there in Chapter 2 is a potential answer: aphasia.
Aphasia is a disruption in expressive or receptive language. It can be as severe as a complete loss of understanding of language, including the inability to speak or think in words. (Aphasia usually affects all forms of language, not just speech.) “Global aphasia” often results from a brain tumor, stroke, traumatic brain injury or degenerative brain disease.
However, milder forms of aphasia are characterized by:
difficulty in finding words (especially nouns, in particular proper nouns)
a tendency to use an incorrect word without a change in sentence structure
In discussing notable case histories of aphasia, Sacks mentions the English writer Samuel Johnson, who experienced aphasia after a stroke at the age of 73. While Johnson eventually regained the ability to speak, he “made uncharacteristic mistakes, sometimes omitting a word or writing the wrong word” in his writing and correspondence.
Adding Up the Evidence
I omit words when I write–more often than the average person it seems–at a rate of about one missing word per one to three hundred words, more if I’m tired (yes, I’ve started keeping track).
The missing words are small but important, like not, an and the. I need to proofread multiple times to catch them, often in an alternative format, because my brain likes to help me out by pretending the missing word exists and skimming right over the omission.
I sometimes use the wrong word without noticing. In writing, it tends to be a word that is close in spelling or sound, though not necessarily in meaning, like bring instead of brain. When speaking, my substitutions are more entertaining. For example, last night The Scientist was using a kitchen towel to clean up a mess.
“Put that in the dishwasher when you’re done,” I suggested helpfully.
He looked at the towel and frowned. “You mean the washing machine.”
Right. That’s exactly what I meant. And what I thought I’d said. This happens a few times a week and I rarely notice that I’ve done it until someone points it out. It’s more common when I’m fatigued or in a setting with a lot of distractions.
I have trouble with retrieving words, especially names of people and things:
“I’ll recycle the, the . . .” I’m staring at the newspaper and pointing at the newspaper and I cannot for the life of me come up with the word for it. All I have is a blank–a tangible, almost physical hole in my mind where newspaper should be. “I’ll recycle that that . . . thing after I finish reading it. $%&*! WHY ARE THERE SO MANY DIFFERENT WORDS FOR THINGS?!”
I’d been attributing the increasing frequency of gaps in word retrieval to getting older. It’s frustrating, especially when I’m trying to find the right word for a written piece and it refuses to surface. Sometimes it will be hours before I can come up with the word I’m looking for; fortunately I’ve learned how to set the problem to process in the background. This often results in me randomly exclaiming things like “dichotomy!” at inappropriate times.
Is Aphasia the Answer?
If this is indeed mild aphasia, then I finally have an explanation for some minor but annoying language difficulties. Perhaps my auditory processing delay is a form of receptive aphasia?
Then again, this could all be tied to Asperger’s. I’ve heard others on the spectrum mention difficulty with finding words at times. Our issues with processing spoken language are widely known. The missing word problem, though? Does anyone else experience that to the degree that I do?
Eager to learn more than what Sacks presents in his brief chapter, I Googled aphasia and instantly regretted it. Here’s what I found at that reliable bastion of truth, Wikipedia:
“Acute aphasia disorders usually develop quickly as a result of head injury or stroke, and progressive forms of aphasia develop slowly from a brain tumor, infection, or dementia.”
Ruh roh.
My language glitches have become frequent enough in the last 2-3 years that I can no longer ignore them. The missing words. The struggle to retrieve words. The odd, unpredictable substitutions. The Scientist says that my receptive language difficulties seem to have gotten worse in the past year too. I ask him to repeat himself a lot, especially when he’s not facing me and I don’t have the advantage of watching his lips.
And this is where I think it pays to stop Googling and back slowly away from the neurology textbook.
The language oddities I’ve described here are firmly in the “inconvenient” category for me right now. Unless that changes, I’ll consider the similarities to aphasia symptoms an interesting bit of trivia. Stay tuned . . .
**In proofreading this multiple times, I found 7 missing words (my, their, a, I’m, an, the and of) and 1 incorrect substitution (ever for even). There may be others that I missed.
This week for Take a Test Tuesday I took the revised Systemising Quotient (SQ-R) test.
Systemizing refers to the drive to understand, construct, predict and/or control the rules of a system. Simon Baron-Cohen, in his desire to wedge autistics into his extreme male brain theory, contrasts systemizing with empathizing as the two primary ways in which humans make sense of their worlds.
The basic premise of the extreme male brain theory is that neurotypical males are better at systemizing and neurotypical females are better at empathizing. Hence, brains can be classified as either male or female according to these aptitudes. Autistic males and females are both better at systemizing, therefore, autistic people have “male brains” and autism is a condition of extreme male neurology.
Using that logic you could also make the case that female basketball players have “male bodies” (i.e. male bodies are on average taller than female bodies, female basketball players have taller bodies on average than females in general, therefore, female basketball players have “male bodies”).
Setting aside the extreme male brain theory, what can we learn from the SQ? The SQ is the subject of several research papers and each time the data show people with ASD generally scoring lower on the EQ and higher on the SQ.
The SQ attempts to measure systemizing in daily life, asking questions about how organized you are when it comes to your financial records, collections or favorite books/music. While the creators tried to avoid introducing bias in terms of subject matter, the test is still vulnerable to this. For example, I want to know the specs of new computer because that’s a topic I’m fairly familiar with.
I’m less interested in the specs of my car’s engine because that’s a subject I know (and care) little about. The same goes for knowing the species of animals and trees or the make-up of committees and governments. Those aren’t subjects I find highly interesting so regardless of how much of a systemizer I am, I’m only going to have a passing curiosity about them
Much of this still relies on personal interests, though perhaps it balances out in the end. The questions about how I bag my groceries and what my closet looks like made me laugh. I bag groceries by type because that makes them easier to put away at home. I hang my clothes in the closet by type so I can find what I’m looking for quickly.
My theory about systemizing? It all comes down to the fact that when you’re autistic, systemizing isn’t simply a preferred way of thinking, it’s a survival mechanism. Without systems and routines, we’d be constantly getting lost in the details.
One final note before we take the test. A lot has been written about gender bias in the EQ and SQ. It struck me as very telling that when the SQ was revised to remove some of the questions that were in “traditionally male domains” and add more questions that might be relevant to females, they removed questions related to investing, religion and culture and added questions related to shopping, cleaning, music and clothing.
Taking the Test
You can take the SQ-R (2005 revised version of the SQ) at the Aspie Tests site. Click on The Systemising Quotient (SQ) link and follow the prompts to get to the test page. I’m assuming you know the drill by now. There are 75 questions and you’re required to choose among strongly agree, slightly agree, slightly disagree and strongly disagree. Positive “strongly” answers score two points and “slightly” answers score one point. Possible scores range from 0 to 150.
It took me a little over 10 minutes to complete.
Scoring the Test
I scored an 85. Not surprising. I’m super organized, have a good memory for details and am insatiably curious about how things work.
I don’t think the SQ is binary in the way that EQ is. For example, on the EQ a positive answer to “I get emotionally involved with a friend’s problems” suggests empathizing. A negative answer suggests remaining detached or perhaps taking a logical problem-solving approach to the friend’s problems. This could be roughly construed as systemizing if we continue to look at it in a strictly binary way.
On the SQ, a negative answer to “I do not follow any particular system when I’m cleaning at home” suggests that one prefers using a system for housecleaning. But what does the opposite answer suggest? Certainly not anything to do with empathizing.
However, the EQ-SQ model sets the two tests up as “complementary” and goes so far as to demonstrate that a composite of EQ-SQ scores is steady across all groups (i.e. my EQ+SQ will be relatively equal to yours and everyone else’s, across all neurotypes). That suggests a strong negative correlation between the two tests.
When you look at the relationship between the AQ, EQ and SQ, it becomes evident that both the EQ and SQ act as a sort of proxy for AQ scores. In other words, they aren’t tests of empathizing and systemizing so much as they’re tests of the traits of autism. Of course autistic people will score higher than average on a test that asks a lot of questions closely related to core autistic traits and lower than average on a test that asks a lot of questions about social skills.
For reference, here are the mean scores from the 2005 SQ-R study:
ASD Male 77.8
ASD Female 76.4
ASD Total 77.2
Typical Male 61.2
Typical Female 51.7
Typical Total 55.6
(I prefer looking at the means from the original studies because the means provided by the Aspie Test site are based on self-reported neurological status, which may not be accurate.)
The Bottom Line
The SQ is an interesting measure of how dependent an individual is on routine, systems and categorization, but the use of the SQ as “proof” of the extreme male brain theory is highly suspect.
The morning of my appointment, I was incredibly nervous. My biggest fear was that I would go through this process and be told that I was officially not autistic–that I wouldn’t come across as “autistic enough” for a clinical diagnosis.
Fortunately, it turned out that I’d found a doctor who has worked with adults enough to know that we have many coping mechanisms and workarounds. He didn’t expect me to present the way a five-year-old boy would. He acknowledged that being an adult autistic doesn’t necessarily mean not attending your cousin’s baby shower; it can mean going to the baby shower and spending a good part of the afternoon hiding out in the kitchen (one of his examples).
The Diagnostic Interview
The first part of my evaluation was a diagnostic interview. I turned in my questionnaire to the receptionist and when Dr. H called me into his office, he’d obviously reviewed it. He started off by asking me to talk about why I suspected I have Asperger’s. I was nervous so I rambled around a lot. Looking back, I probably should have looked at my notes and used them as a guide, but my brain was going a hundred miles an hour.
Once my initial thoughts fizzled out, Dr. H. started working through the questionnaire, confirming symptoms I’d answered positively and asking clarifying questions. As I relaxed a little, the conversation became less structured. We talked a lot about my childhood, with the doctor encouraging me to give examples or tell stories to illustrate certain points. Gradually, he began inserting comments about Asperger’s, explaining how some of my symptoms were typical and how they fit into the diagnostic picture.
The interview lasted about an hour. By the end of it, I felt like we’d hit on all of the key points I wanted to talk about as well as some that I hadn’t considered important. Dr. H concluded the interview by explaining that he wanted to evaluate me for ASD, ADHD and Social Anxiety Disorder. The second one was a surprise but I was glad that he was forming his own hypotheses in addition to the one I’d presented.
He then explained a little about how cognitive testing works and about the qualifications of B, the ASD testing specialist who would administer the tests.
The Part Where I Provide Plenty of Autistic Behavior for Observation
When we moved to B’s office, I got a chance to demonstrate two of the symptoms I’d described in the interview: face blindness and delayed auditory processing. Dr. H introduced me to B and she cheerfully said, “Yes, we already met–you asked me where the restroom was when you came in.”
Completely thrown by the fact that I didn’t recognize her, I said “Really? Okay.”
As I was kicking myself for that useless reply, Dr. H asked, “Got plurdled gabbleblotchits on a lurgid zoo?”
I reflexively replied, as I always do when I have no idea what someone has said, “Sorry?”
“What would you like to be called?” he repeated.
I probably could have gone home at that point because not recognizing that I’d already met B, not being able to smooth over the awkwardness that followed, not greeting her with my name, not understanding what Dr. H was saying, being more focused on orienting myself in the room than connecting with the person I was going to work with–in less than 60 seconds, I’d exhibited a boatload classic autistic behavior, much of it as a result of struggling to switch activities/environments, which is in itself textbook.
To her credit, B quickly put me at ease. She spent about ten minutes “getting ready” while I sat, mostly silent, and studied the colorful barcode prints on her wall. Honestly, I wouldn’t be surprised if the time she’d spent puttering around with her supplies was more for my benefit than hers. By the time we started on the cognitive testing, I was feeling reasonably focused again.
This post is a part of today’s “Autistic people are . . .” flashblog. You may have seen the news this week that Google has promised to eliminate the problematic “Autistic people should” autocompletes in response to last week’s flashblog. They’ve said it will take time to engineer, so while the hateful autocompletes are still appearing, hopefully they’ll soon be gone.
We can make a difference by speaking up.
——-
Autistic people are everywhere.
We sit next to you at school and on the bus. We give your dog his rabies shot, teach your kids, make your latte and sweep the floor at your grocery store. We pass you on the sidewalk and stand beside you on the subway. We eat in the same restaurants, shop in the same stores, go to the same gyms that you do.
We are mothers and fathers, husbands, wives and partners. We are sons and daughters, sisters and brothers, aunts, uncles and grandparents.
We are everywhere, all around you.
*
If you don’t see us, it’s because we’ve mastered the art of hiding in plain sight.
We don’t come neatly labeled. Many of us don’t “look” autistic. You can interact with us and not realize you’ve talked to, worked with, studied with, played with, cursed out, fallen in love with, or are related to an autistic person.
We often don’t share our neurological status unless we feel that we absolutely have too, and even then sometimes we don’t.
There is no payoff for calling attention to our differences. There is no reward for being openly autistic. The risks are real.
Many of us remain quietly, even silently, autistic.
We are everywhere, sitting beside you, walking past you, interacting with you. Do you see us?
I’ve been thinking and reading a lot about anxiety recently. When I was diagnosed with Asperger’s, I was also diagnosed with Social Anxiety Disorder.
Here’s how I feel about that: Social Anxiety? Yes. Disorder? Not so much.
Disorder implies that my social anxiety is irrational. Is it? Consider this:
“Anxiety at appropriate levels is important for adaptive functioning. There are many environmental hazards that must be avoided and these are often learned through the process of anxiety induction. The resultant anxiety response is learned through the association of certain stimuli with unpleasant consequences.” (from “Autism and the Physiology of Stress and Anxiety”, Romanczyk and Gillis)
Anxiety, like fear, protects us from danger. It raises our guard and makes us wary. In this way, it’s healthy. Without it, we might be less motivated to get an education, to work, to care for our loved ones and ourselves.
What is Anxiety?
Anxiety is a state of worry, concern or dread related to something that hasn’t yet happened and may, in fact, never happen. Think about some things that we typically feel anxious about:
committing to a relationship
giving a major presentation for school or work
becoming a parent
meeting a partner’s family
starting a new job
learning to drive
flying on an airplane for the first time
traveling in a high crime area
When you feel anxious about an upcoming event, you spend more time thinking about it and preparing for it than you would for a more mundane activity. You examine the possible consequences and give extra attention to your actions to ensure the best possible outcome. Anxiety heightens your awareness; heightened awareness sharpens your focus, increasing your safety.
It’s important to note that here and throughout this piece, when I talk about anxiety, I’m referring to appropriate levels of anxiety, not paralyzing anxiety. An appropriate level of anxiety is one that is manageable. I feel nervous in the days before giving an important Powerpoint presentation, but I manage my anxiety and complete the presentation to the best of my ability. An inappropriate level of anxiety is one that prevents a person from completing a necessary or desired activity. For example, if I got so anxious about the presentation that I ended up sick in bed, fainted in the conference room, or lied to avoid presenting.
Not all anxiety is healthy and it’s important to recognize where your anxiety falls on the healthy/unhealthy continuum.
The Function of Social Anxiety in ASD
So that’s how anxiety works in the typical brain. But what about in the autistic brain?
From childhood, autistic people know that we’re missing key information in social situations. We often have difficulty interpreting facial expressions, tone of voice, body language, and non-concrete speech. Some people also struggle with auditory processing and sensory overload in public or group settings.
The results of our social communication challenges can range from inconvenient (missing a joke or not following a conversation) to dangerous (being bullied, taken advantage of or assaulted). There are also negative health consequences–many autistic people need hours or days to physically recover from prolonged or intense social interaction.
Over time, “through the process of anxiety induction,” we realize that certain social situations are “environmental hazards that must be avoided” (as Romanczyk and Gillis described). In other words, because of a very real hazard, we develop anxiety that for us has a very real cause. It isn’t disordered. It’s a defense mechanism, developed through “the association of certain stimuli with unpleasant consequences.”
Social anxiety is, therefore, not only “important for adaptive functioning” in autistic people, it’s essential.
Red Light, Green Light
Autistic social anxiety is not the same as neurotypical social anxiety. If a person with intact social communication abilities has severe anxiety about social situations, then they have a disorder because their fear is irrational. When a person with impaired social communication abilities has anxiety about social situations, they are like a poor swimmer who is anxious about boarding a boat. The perceived risk is real and rational.
If fear is a red light–a glowing “stop” signal in our brain–then anxiety is a yellow light. It’s the feeling that says, “slow down, caution, stop and pause a moment before continuing down this road.”
We should heed this feeling, not cure ourselves of it.
Appropriate vs. Inappropriate
But, some will say, too much social anxiety and you’ll become a recluse! A hermit! The little old lady shouting at those darn kids to get off her lawn!
Well, yes and no. First of all, allow me to horrify the more socially oriented among you by saying this: people aren’t all that interesting and the rewards of socializing are sometimes overrated. Consider the possibility that all of the following (fictional) people are meeting their needs for social interaction:
the person who lives alone, works at home and in the evening participates in role-playing games, an acting workshop and a drumming circle
the person who lives with a partner and has lunch once a week with a close friend
the person who attends classes full-time and prefers to socialize online in text-based formats outside of class hours
the person who chooses to spend time at home with family and only goes out for necessary errands or events
the person who works around people all day and likes to spend their evenings alone
The social preferences of these people may differ from the majority of their peers, but they aren’t exactly in Grey Gardens territory.
Being anxious about socializing is not the same as completely avoiding social situations. It’s possible to manage social anxiety in the same way we manage anxiety about other things. Someone–NT or autistic–might feel anxious about starting a new job, but that doesn’t mean they won’t do it. Most people have strategies for managing anxiety and autistic people are no different.
What is different is that our social anxiety is automatically pathologized and then “treated” with therapy or medication. We’re told that our fear is irrational and we need to change the way we “think about” social interaction. We’re told that if we just “relax a little” we’ll find social interaction much more enjoyable.
What would be far more helpful is to acknowledge our anxiety as valid and support our right to socialize at our preferred level, in our preferred ways, without being stigmatized for it.
What Anxiety Tells Us
So how does social anxiety keep us safe?
First there is the obvious example: when you have difficulty interpreting nonverbal cues, it can be hard to know when another person is a threat. This can be especially true for autistic women and girls, increasing our chances of becoming the target of sexual assault, sexual abuse or domestic violence. The autistic woman who feels anxious about dating, intimate relationships or venturing into unfamiliar situations has good reason to–the statistics for violence against autistic women are alarming.
Autistic people are also often victims of bullying. The autistic boy or girl who is anxious about recess or the school bus has a large databank of negative interactions feeding that anxiety. Their anxiety tells them that unstructured activities with limited adult supervision are a potential danger zone.
Those are both reasonable examples, right? But what about the anxiety-inducing holiday party, trip to the mall, or vacation? Surely that’s irrational?
Not if you’re forced to think about every social activity in terms of cost. There are many analogies for this concept: spoon theory and the social cup vs. bucket analogy are the most popular. I’ll spare you a new analogy and give you an example instead.
Last spring my nephew and his wife came to visit for a long weekend. He’s one of my favorite nephews and I was looking forward to meeting his new wife. Still, I was anxious. Having two additional people in the house for three days would mean a disrupted schedule, unfamiliar noises and smells, a loss of my precious alone time and lots and lots of talking.
The Scientist and I came up with a schedule–scheduling is essential for me to get through three days of company–and then I set about thinking of ways to conserve my resources. I volunteered to drive because I find it relaxing. We scheduled downtime for me on Saturday afternoon while everyone else went out. I suggested we visit a historical site that I knew well, because it would mean a familiar environment plus the chance to infodump in a socially acceptable way.
We had a great time. They enjoyed the places we visited and the meals I cooked. We laughed a lot and had meaningful conversations. Things couldn’t have gone better. And still, Saturday night as everyone sat around the dinner table talking for hours after the meal was finished, I found myself shaking uncontrollably.
Even with all of my planning, even though I was enjoying myself, the day’s socializing had overwhelmed me. I knew it was coming, had felt myself shutting down as the evening wore on, but I ignored the warning signs. I didn’t want to end a great day on a bad note.
Unfortunately, it’s not about what I want. Social interaction has a real physical cost for autistic people. If I don’t listen to the voice of caution in my head and limit my interactions, my body will eventually take over and limit them for me.
When I’m in a situation where I feel comfortable, I can handle longer interactions. If I have to deal with unstructured activities, unfamiliar places, new people, rapid shifts in conversation partners or topics, or any of a long list of other things I find challenging, I’ll hit my limit sooner. An hour might be all I can deal with before I start feeling a strong need to escape.
Since being diagnosed with Asperger’s, I’m getting better at “reading” myself. The anxiety, the need to escape, the withdrawal that precedes the uncontrollable shaking–these are not things I need to be cured of. They are signs that I need to take care–yellow lights to be heeded–and I’m learning to listen to them.
This week for Take-a-Test Tuesday I took the Cambridge Mindreading Face-Voice Battery (CAM) which is another test of the ability to recognize emotions in others.
The Cambridge Mindreading Face-Voice Battery (CAM) tests recognition of complex emotional states. It consists of short audio and video clips in which actors convey 1 of 20 different complex emotions through either their voice or their facial expressions.
The theory behind the CAM is that autistic people are able to read basic emotions but have difficulty interpreting complex emotions. Basic emotions are the ones that we learn early in life: happy, sad, angry, surprised. Most people learn these by age 6.
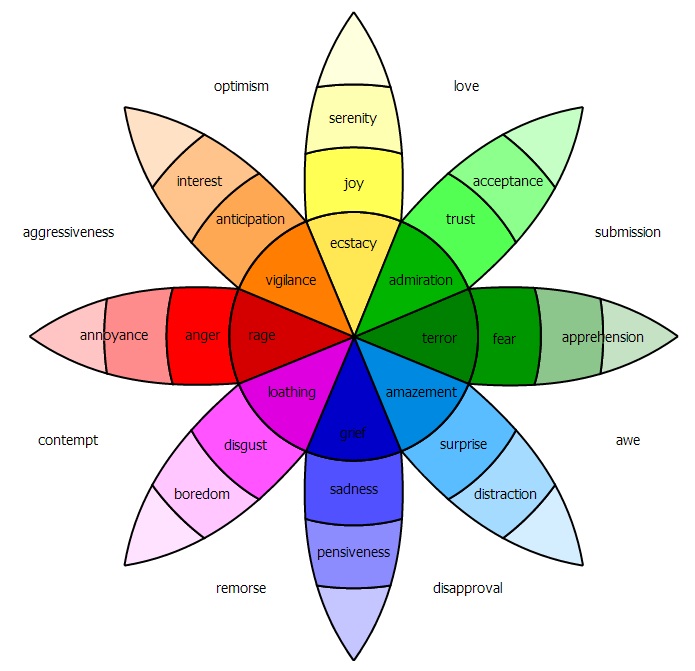
Complex emotions are sometimes described as combinations of basic emotions or as basic emotions plus cultural conditioning. They include mental states like stern, intimate, guarded, admiring, submissive and vibrant. There are hundreds of complex emotions and it takes us years to learn them. Generally, most people can recognize the majority of complex emotions by the time they reach adulthood.
Robert Plutchik’s Wheel of Emotions is one of many ways of thinking about the relationships between basic and complex emotions
According to the CAM creators, the emotional states presented in the clips are “higher order” emotional concepts:
6 concepts from level 4 (concepts understood by typical 15–16 year olds)
13 concepts from level 5 (understood by typical 17–18 year olds)
1 concept from level 6 (words understood by less than 75% of typical 17–18 year olds)
The purpose of the test is to examine whether autistic people grasp these more complex emotional states. It includes both negative and positive emotions as well as subtle and intense emotional states. Each of the 20 emotions is repeated 5 times.
Taking the Test
The Face-Voice Battery has two parts. Part 1 consists of listening to 50 short clips of actors saying a phrase or sentence. You’re given 4 options for describing the emotional content of the clip. Part 2 consists of watching 50 3-5 second videos of actors silently portraying facial expressions. Again you’re given 4 options that describe the emotional content.
You can take the Cambridge Mindreading (CAM) Face-Voice Battery at aspietests.org. To begin, click on the The Cambridge Mindreading Face-Voice Battery – Part 1 (Voices) link. After entering your age and diagnostic status and accepting the terms, you can proceed to the voice clips. As you take the test, keep in mind that speed counts. In addition to a %-correct score, the test returns an “average time to answer” score. Part 1 took me about 10 minutes to complete.
Once you finish Part 1, click the “back to the homepage” link and then click the Cambridge Mindreading Face-Voice Battery – Part 2 (Faces) link to begin Part 2. Again, speed counts. This part took me about 10 minutes to complete as well.
Scoring the Test
I did well on this test–in fact, I matched the mean score of neurotypical females in the original research study. Here is my score:
You scored 90.0% in 5.7 seconds. Faces: 84.0% (42 correct) Voices: 96.0% (48 correct)
NT Faces task: 44 correct (88%)
NT Voice task: 43 correct (86%)
NT Total: 86 correct (86%)
I’m not surprised by how well I did on the voices portion of the test. “Voice data” is my primary means of reading social situations. It helped that the informational content of the phrases matched the emotional content of the voices. For example, when I heard “that is horrible” I took into account the information being conveyed by the statement as well as the tone of voice to settle on my choice of “appalled.” This is considered a “strategy” by the test creators, so basically, once again, I’m “cheating.” But it works, so hooray for adaptations.
The video clips were a mixed bag. I think I did better on the ones that had a dissimilar set of possible answers (i.e. appalled, vibrant, blank, or intimate) and the ones that I remembered to glance at the answer choices before the clip played.
As an experiment, for some trials I watched the clip and tried to form an answer before looking at the choices. On one video, I was certain the answer was “sarcastic” but that wasn’t one of the choices; I think the correct answer was “reassured.”
A few other random thoughts:
Am I the only one who thought most of the voice clips sounded like they were straight out of Dickens novel?
The use of live action videos is more realistic than static photos, but I still didn’t feel like the test results were reflective of my real life ability to read emotions.
I liked seeing the contrast in my voice vs. facial expression reading skills.
Some of the video clips made me incredibly uncomfortable to the point that I had to glance away.
I couldn’t find any data on the “time to answer” scores. From background reading about this type of test, I know that researchers often use the average time to answer as a metric to gauge competency. The assumption is that the longer it takes to answer, the more processing your brain is doing to produce an answer.
The Bottom Line
CAM feels more realistic than Reading the Mind in the Eyes, but it’s still far from an accurate test of the fluid way that emotions present in real life interactions.